

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Bone morphogenic protein-2 (BMP-2) is a potent osteoblastic differentiation factor of mesenchymal progenitor cells and enhances new bone formation [1,2]. Regenerative therapy using BMP-2 has been widely studied in protein therapy with recombinant human BMP-2 as well as BMP-2 gene therapy [3-7]. Since BMP-2 gene therapy can induce the sustained expression of BMP-2 synthesized in vivo, BMP-2 gene therapy can produce positive results for unfavorable bone healing conditions such as a critically sized defects (CSDs) [8,9].
In the measurement of regenerated bone tissue in BMP-2 gene therapy, most studies have performed histological examination [10,11]. For histomorphometric analysis to measure the newly formed bone tissue, a representative histology of each sample was examined using a coronally sectioned slide at the center of the defect. Although the histological examination provides precise information about the regenerated bone, the information is limited to only one slide at the center of the defect. Therefore, histological examination alone could be insufficient to evaluate the status of entire defects sites.
Recently, micro-computed tomography (micro-CT) has been performed to observe the bone regeneration at the entire defect sites [12-14]. Using a computer program to convert micro-CT images to 3-dimensional form, all the regenerated bone in the defects can be observed. In addition, information about the newly formed bone such as the bone mineral density or percent of the bone volume could be obtained via a micro-CT analysis program [12,15]. While the validity and reliability of micro-CT has been reported in previous studies [16,17], no report has addressed which factor affects the correlation between micro-CT analysis and histomorphometric analysis. Moreover, the optimal threshold level for detection of the newly formed bone tissue at the calvarial defect was not determined.
This study aimed to evaluate the correlation between micro-CT analysis and histomorphometric analysis in rat calvarial defects treated by BMP-2 ex vivo gene delivery. The factors affecting the correlation between both analyses were examined and the optimal threshold level for detection of the newly formed bone was evaluated. With these objectives, 8-mm critically sized bone defects were made in the rat calvaria, and autogenous rat bone marrow stromal cells (BMSCs) transfected by adenovirus containing BMP-2 gene delivered at the defects.
MATERIALS AND METHODS
Animal models
A total of 24 male Spraque-Dawley rats (8 weeks old) were used in this study. The animal research protocol was approved by the Institute of Laboratory Animal Resources, Seoul National University. The animal experiments were conducted according to the guidelines established by the Seoul National University Institutional Animal Care and Use Committee.
Preparation of autogenous rat BMSCs
Two weeks before calvarial surgery, autogenous rat BMSCs were harvested from both tibia under general anesthesia. The harvested BMSCs were cultured in the media of α-minimum essential medium (MEM) supplemented 10% (v/v) fetal bovine serum (FBS) (Gibco, Grand Island, NY, USA) and 1% (v/v) penicillin-streptomycin solution (5,000 U/mL penicillin and 50 µg/mL streptomycin) (Gibco) at 37℃ in a humidified atmosphere of 95% air and 5% CO2. Media changes were done twice a week. When the cells reached confluence, the cells were released with 0.25% trypsin/1 mM ethylenediaminetetraacetic acid (EDTA). The cells of two or three passages of cells were used for transduction.
Adenoviral vector construction and transduction
Replication-defective human Ad5 containing the cDNA for human BMP-2 (ATCC, Manassas, VA, USA) in the E1 region of the virus (AdBMP2) was constructed by in vivo homologous recombination. Briefly, an expression cassette encoding the BMP-2 gene was amplified in Escherichia coli and ligated to Adeno-X Viral DNA (BD Biosciences, San Jose, CA, USA). Recombinant adenoviruses were obtained from human embryonic kidney 293 cells transfected by recombinant Adeno-X vectors. The rat BMSCs were plated at a density of 1×106 cells/cm2 and transduced with AdBMP2 in α-MEM supplemented with 10% FBS and antibiotic-antimycotic solution. The virus was allowed to adsorb for 4 hours and the media was then added. Expression of BMP-2 by AdBMP2-transduced rat BMSCs was quantified by enzyme-linked immunosorbent assay (Quantikine BMP-2 microplate, R&D systems Inc., Minneapolis, MN, USA).
Surgical procedures
General anesthesia was induced by a combination of an inhalation of isoflurane and intramuscular injection of ketamine and xylazine. A midline incision was made over the calvarium and a full-thickness flap was elevated. An 8 mm critically sized calvarial defect was created using a trephine bur (3i Implant Innovation, Palm Beach Gardens, FL, USA) under sterile saline irrigation. The animals were divided into three groups as follows: 1) collagen gel (control group), 2) non-transduced autogenous rat BMSC mixed collagen gel group (BMSC group), 3) AdBMP-2 transduced autogenous rat BMSC mixed collagen gel group (BMP-2 group). Collagen gel was prepared with 1% collagen (MATRIXEN-PSP, Bioland, Cheongwon, Korea), 10-3 N HCl, 26 mM NaHCO3, 20 mM HEPES, 0.025 N NaOH with cells according to the experimental group before the surgery. The flaps were sutured by layers with 5-0 chromic gut and 4-0 silk. All the animals received a single intramuscular injection of cefazolin.
Micro-CT
Four rats of each group were sacrificed at 2 and 4 weeks after surgery, respectively. The tissues including the surgical sites were harvested and fixed in 10% neutralized-buffered formalin solution and micro-CT was taken using Skyscan 1172 (SkyScan, Kontich, Belgium). Through a computer analysis program, the percent of bone volume in the whole defect site was calculated (CT analyzer, SkyScan). The measurement was repeated at each 50, 60, 65, 70, and 80 grayscale index of the lower grey threshold level for determination of the optimal threshold level. The automatically set threshold level in analyzing program was 65.
Histological procedure
After micro-CT taking, each sample was decalcified with 10% EDTA solution for 2 weeks and dehydrated through a series of ethanol solutions of increasing concentration and embedded in paraffin. Coronal sections 5 µm thickwere obtained at the three regions: the anterior 1/3 position, center, and posterior 2/3 position of the circular defects. Among them, the coronally sectioned slide at the center was defined as the representative histology. Each specimen was stained in hematoxylin and eosin. After microscopic examination, a photograph of each specimen was taken with a digital camera and was used for histomorphometric analysis using a computer analysis program (Tomoro Scope Eye 3.5 Image Analyzer, Techsan Digital Imaging, Seoul, Korea). Regeneration of bone was quantified by calculating the percentage of the new bone area out of the whole defect area. The whole defect area was measured arbitrarily by the area surrounded by two imaginary lines along the inner and outer calvarial bone contour and both sides of defect border.
Statistical analysis
Statistical analysis was performed using a computer program SPSS ver. 18 (SPSS Inc., Chicago, IL, USA). Two-way analysis of variance (ANOVA) was conducted to compare the new bone formation of each group in both histomorphometric analysis and micro-CT data analysis. A Student's t-test was performed to compare the new bone formation of each group between 2 and 4 weeks. Using a paired t-test, the result of histomorphometric analysis from one representative section was compared to the results from the 3 sections. To evaluate the correlation between histomorphometric analysis and micro-CT data analysis, a Pearson's correlation coefficient test was performed at first and high correlation coefficient values were obtained. Subsequently, a linear regression analysis between both analyses was performed to determine the optimal threshold level for the micro-CT data analysis. Additionally, a repeated measures ANOVA was performed to observe the change in the pattern of the bone volume measurements with increasing of the lower threshold level. The statistical significance level was P<0.05.
RESULTS
Histology and micro-CT images
The representative histology of each group was examined, at first. As shown in Fig. 1, the BMP-2 group showed remarkable bone formation at 2 weeks although the newly formed bone was sponge-like woven bone. At 4 weeks, the BMP-2 group also produced lots of newly formed bone, which was more mature than at 2 weeks. The BMSC group showed slight new bone formation at 2 weeks and new bone formation had increased by 4 weeks. In the control group, a collagen remnant and slight new bone formation was observed at 2 and 4 weeks. From histomorphometric analysis, in the BMP-2 group, the new bone formation was found to be 76.21±26.24% at 2 weeks and 55.20±7.60% at 4 weeks, and it was significantly different from the other groups (P=0.026, P=0.034) (Table 1). There were no significant differences between the values at 2 and 4 weeks in any of the groups.
To compensate for the limited information from only one section, two additional histological sections at the anterior 1/3 and posterior 2/3 region, as shown in Fig. 2, were taken from each sample. A mean value of measurement from 3 sections was used as a representative value of each sample and it was highly correlated to the new bone area measured from a representative histology (adjusted r2=0.845, P<0.001). However, in the BMP-2 group, there was a significant difference at 2 weeks between measurement from 1 section and from 3 sections (P=0.004).
Micro-CT reconstructing a 3-dimensional view showed a result similar to that from the histomorphometric analysis (Fig. 3). A 3-dimensional image was obtained with the automatically set-up threshold level (lower grey threshold level=65). The defect fill of the BMP-2 group at 2 and 4 weeks was greater than that of the other groups. At 4 weeks, the BMSC group showed more bone fill than at 2 weeks.
Correlation between Micro-CT analysis and histomorphometric analysis
Since the threshold level influences the new bone detection, the bone volume was repeatedly measured with the lower threshold level set at 50, 60, 65, 70, and 80 (Fig. 4, Table 2). As the lower grey threshold level was increased, new bone volume generally decreased. The bone volume measured from micro-CT in the BMP-2 group was significantly greater than in the other groups at all threshold levels, similar to the histomorphometric analysis (P<0.001 for all cases).
The volume (%) of new bone from micro-CT analysis was highly correlated with the new bone area (%) obtained from the histomorphometric analysis of the representative histology (P<0.001) (Fig. 5). As a result of a linear regression analysis, the bone volume of micro-CT measured at the threshold level of 50 was highly correlated to the new bone of histomorphometric analysis (adjusted r2=0.846, P<0.001). As the threshold level was increased, the correlation between the micro-CT analysis and histomorphometric analysis decreased.
The bone volume measured from micro-CT was also highly correlated with the new bone of the histomorphometric analysis of 3 sections (P<0.001), and the correlation was the highest at the threshold level of 50 (adjusted r2=0.824, P<0.001) (Fig. 6).
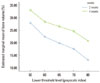
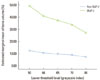
At 2 weeks, the histomorphometric analysis and micro-CT analysis were the most highly correlated at the lower threshold level of 50 with adjusted r2=0.907 (Fig. 7). At 4 weeks, the correlation between the two analyses was decreased than at 2 weeks and the influence of the lower threshold level on the measurement was disappeared (Fig. 8). The new bone volume of overall samples at 4 weeks was higher than at 2 weeks and it was decreased as the lower threshold level increased with a similar slope to 2 weeks (Fig. 9). At 2 weeks, the bone volume of the BMP-2 group was sharply decreased as the lower threshold level increased and the reduction pattern was significantly different from the other groups (P<0.001). The BMP-2 group at 4 weeks also showed a significantly steeper reduction pattern than the other groups (P<0.001). The BMSC group had a higher bone volume than the control group although the reduction pattern was similar to the control group (Fig. 10). Regardless of timing, as the threshold level increased, the BMP-2 group with a great deal of new bone formation also had a significantly steeper reduction pattern than the non-BMP-2 groups, which showed only slight bone formation (Fig. 11).
DISCUSSION
For the evaluation of new bone formation in regenerative therapy, most studies have been performed using histomorphometric analysis, which is limited to 2-dimensional information from a representative slide. Therefore, recent reports have also performed micro-CT, observing the newly formed bone of the entire defect site using 3-dimensionally reconstructed images [8,18]. In the present study, the amount of new bone measured from histomorphometric analysis and from micro-CT analysis was highly correlated in regeneration therapy with BMP-2 gene therapy on rat calvarial defects. This result was similar to previous studies. Maréchal et al. [19] reported a strong correlation between micro-CT and serial histological sections of bone augmentation under a titanium barrier membrane with r2=0.072. Umoh et al. [20] compared the histological assessments and in vivo micro-CT images in a rat calvarial model and also observed a high correlation between both examinations with r2=0.70. Kochi et al. [21] also reported consistent patterns of bone formation in both analyses in bone augmentation with hydroxyapatite.
In the present study, the adjusted r2 value of linear regression analysis was greater than in other studies although the direct comparison to previous studies has been limited. This is related to the threshold level used in each experiment. The present study showed that the correlation between both analyses was highly dependent on the lower threshold level. At the lower threshold level of 50, the most significant correlation was observed, and the adjusted r2 value decreased as the lower threshold level increased. This phenomenon was maximized in the BMP-2 group. In the histology at 2 weeks, the new bone was the immature and sponge-like woven bone, contrasting with the matured bone with lamellar bone and marrow space at 4 weeks. Therefore, the bone volume measured from micro-CT was highly influenced by the threshold level at 2 weeks in BMP-2 group. At the lower threshold level of 50, the immature bone tissue with low radiopacity could be detected despite of an increase of the background noise. Since the newly formed bone at 4 weeks was mature enough to detect in the radiology, the new bone volume measured from micro-CT analysis was not sensitive at the change of the threshold level. Therefore, the optimal threshold level of the micro-CT analysis should be determined according to the purpose of the study. To observe the new bone formation in the early period, a low lower threshold level was advantageous for the measurement of immature new bone despite of possibility of false positives. On the other hand, to distinguish the mature bone, micro-CT analysis using a higher threshold level could be proper during the evaluation of the newly-formed bone.
Despite of the high correlation between two analyses, the difference in the new bone area from histomorphometric analysis between 2 and 4 weeks was greater than that from micro-CT analysis. Because some newly formed bone of the BMP-2 group was mixed with collagen gel, the border between them was not clear in histological examination and possibility of false positives existed. Since measurement using micro-CT analysis detects only the mineralized bone, the measurement the bone volume obtained from micro-CT is also helpful in judgment of the histomorphometric analysis.
Micro-CT has some advantages in the bone research; the sequential data through in vivo micro-CT could be obtained from individual animals during the research period and the number of animals could be reduced. Additionally, micro-CT data could be acquired rapidly without a destructive and time consuming process related to the histological examination. Micro-CT analysis has been compared to the alternative methods for histology, and it could be a good monitoring method highly correlated to histomorphometric analysis of bone regeneration during a study.
In this study, new bone formation at 2 and 4 weeks was analyzed using histomorphometric analysis and micro-CT analysis. Since this study was focused on the methodological aspect of new bone formation using BMP-2 gene therapy, this interval was effective for the comparison of the early woven bone and lamellar bone. However, this interval could be insufficient for evaluating the effect of genetically modified rat BMSCs overexpressing BMP-2 in new bone formation. In previous studies about the regenerative therapy, a longer time interval such as 4 and 8 weeks was used to compare bone regeneration therapy methods in rodent models and further study will be needed to evaluate the new bone formation in BMP-2 ex-vivo gene therapy.
In conclusion, the new bone measurement using histomorphometric analysis and micro-CT analysis was highly correlated, especially at the low threshold level in the early period. The bone volume measured from micro-CT of the BMP-2 group was more sensitive to the changing of the lower threshold level than the other groups.











 XML Download
XML Download