

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Suturing, which is the final procedure of a surgery, is used to reattach the removed tissue, to control bleeding, and allow for primary healing [1]. In addition to the physical requirements for an ideal suture, such as maintaining proper form, ensuring the ease of sterilization and manipulation, and maintaining ligation and tension, the biological requirements of proper absorption time and minimum tissue response have also been suggested [2]. In intraoral surgeries, a variety of suture types have been applied [3]. Sutures can be divided into absorbable and non-absorbable ones and are classified as monofilament or multifilament types. Although microbial inflammation response due to the multifilament interstices has been demonstrated, silk has been widely used in intraoral surgeries because it has the advantages of easy manipulation, the capability of maintaining knot security, and less irritation than nylon [4,5]. Polyglycolic acid, a polymer of lactide and glycolide, is used to manufacture an absorbable suture. After being extracted as a melted polymer, a thin fiber is manufactured into a braided form to improve its ease of manipulation. Polyglycolic acid is absorbed in 60 to 90 days after insertion. It is hydrolyzed without any phagocytosis, which results in a weaker immune response than that of absorbable organic sutures [6]. One of the well-known non-absorbable monofilaments, nylon, is made from polyamide polymer and has been reported to show a high resistance to infection, high tension, and a low acute inflammation reaction [7].
Due to the oral conditions of moisture and susceptibility to infection by saliva, ingested food, microorganisms, etc., a suture placed in an oral cavity is affected differently than a suture in extraoral conditions [8]. In addition to the chronic inflammation response, a suture placed in an infectious condition is likely to show constant acute inflammation responses. Furthermore, as a result of the inflammation response due to the suture itself, a suture can interfere with optimal wound healing and can result in the formation of excessive scar tissue, thereby reducing the tensile strength of the wound site. This eventually negatively affects the immune response to infection. Therefore, the immune response to a suture is an important factor when choosing the proper suture type [9,10].
The suture type is one of the critical factors influencing infection occurrence post-surgery. It has been reported that braided sutures show a more severe inflammation reaction than do those without any braid, due to the potential for penetration and transfer by microorganisms [11,12]. On the other hand, it has been suggested that wound infection is not always associated with suture structure, but may also pertain to the number of fibers [13]. In addition, Gabrielli et al. [14] insisted that patient factors such as age and gender have an influence on the immune response and infection occurrence rate when they observed no significant differences in immune response among sutures.
Studies on suture-induced immune response according to oral mucosa tissue type have been conducted. Castelli et al. [15] observed that the inflammation due to a suture located on the buccal mucosa was more severe than that of a suture located on the gingival mucosa. However, it was reported that there was no significant difference in immune response between the gingiva and alveolar mucosa in an adult dog [8].
The purpose of this study was to compare and evaluate the inflammatory responses induced by the three suture types widely used in clinical dentistry in the keratinized gingiva and buccal mucosa of beagle dogs.
MATERIALS AND METHODS
Surgical procedures
The sutures applied in this study were classified into monofilament and multifilament types. The multifilament sutures included silk (size 5-0, reverse cutting needle FS-2, Ethicon Inc., Somerville, NJ, USA) and polyglycolic acid (coated Vicryl, size 5-0, reverse cutting needle FS-2, Ethicon Inc.), while the monofilament, nylon (size 5-0, reverse cutting needle FS-2, Ethicon Inc.) was also used.
Four one-year-old beagle dogs bred in isolated conditions and provided with a soft diet to protect the suture application site were used in this study. The experimental protocol (KHMC-IACUC 08-013) was approved by the Institutional Animal Care and Use Committee of the Kyung Hee University.
General anesthesia was conducted with the combination of 2 mL tiletamine and zolazepam (Zoletil, Virbac, Carros, France) and 0.5 mL xylazine (Rompun, Bayer Korea Ltd, Seoul, Korea) by intramuscular injection. The mandibular premolars (P1-P4) were extracted under local anesthesia of 2% lidocaine with 1:100,000 epinephrine (Lidocaine HCl, Huons Co., Seoul, Korea) by a sulcular incision and flap elevation approach. The extraction sites were sutured with an absorbable suture (plain gut, size 4-0, cutting needle P426, Ailee, Seoul, Korea). After a healing period of two months, the keratinized gingiva of the edentulous mandible and the buccal mucosa of the maxilla were sutured by single sutures of silk, polyglycolic acid, and nylon under general anesthesia. The sutures were inserted with minimal tissue tension, maintaining constant intervals and depth with a minimum suture gap of 7 mm. During the three days after single suturing, intramuscular injections of 2 mL gentamicin (Dongwha Pharm Co., Seoul, Korea) and 0.5 mL ketoprofene (Uni-Ketopro, UNIBiotech, Seoul, Korea) were administered. Three, seven, and 14 days subsequent to the single sutures, the tissue specimens were derived. During the entire experimental period, daily irrigation of normal saline and swabbing with 2% chlorhexidine were performed for plaque control.
Specimen preparation and observation
The sutures and surrounding tissues were retrieved en bloc, fixed with 10% neutrally buffered formalin solution, and subsequently embedded in paraffin. After the dissection of the specimens with a thickness of 8 µm, the specimens were double stained with hematoxylin and eosin for histopathological evaluation under a light microscope (BX-51, Olympus, Tokyo, Japan). Photography and analysis of the specimens were performed with a digital camera (DP-71, Olympus).
Statistical analysis
A modification of the method described by Racey et al. [16] was used to evaluate the inflammatory reaction. The density of 3 cell-types (polymorphonuclear leukocytes, lymphocytes, macrophages) was counted and assigned a numerical grade from 1 (bare scattering) through 3 (dense aggregation).
A two-sample t-test was used to determine the inflammatory grade difference between the groups in the keratinized gingiva and buccal mucosa. To measure the statistical significance of the inflammatory grade according to time point, one way analysis of variance and Duncan's method for post-hoc testing were performed (P-value<0.05).
RESULTS
Immune response to silk sutures
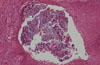
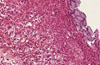
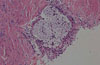
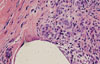
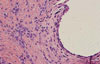
Seven days after suturing, severe infiltration of inflammatory cells was noticed around the sutures (Fig. 1). Fourteen days post-suturing, a moderate degree of inflammatory cell infiltration and epitheloid formation were observed around the sutures. In the epithelium surrounding the sutures, a low degree of inflammatory cell infiltration was observed (Fig. 2). For the suture located on the buccal mucosa, a more significant inflammation response was noted (Fig. 3). During the entire study, the group sutured on the mandibular keratinized gingiva showed only a slight inflammation response, compared with the sutures on the buccal mucosa. There was no difference in the inflammation response among the groups as time progressed.
Immune response to polyglycolic acid sutures
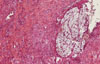
Until 14 days after suturing, absorption of the suture was not observed, and the suture interstices were maintained. Three days after suture, the inflammatory cell infiltration and immune responses within the surrounding epithelium and connective tissue of the mandibular keratinized gingival suture group were weak (Fig. 4). Seven days post-suturing, extensive inflammatory cell infiltration was observed surrounding the sutures and within the connective tissues of both groups. In addition, neutrophils and leukocytes were observed, along with the formation of bacterial plaque (Fig. 5). The immune response after 14 days had similar histologic features to that after seven days. While the tissues surrounding the sutures showed a moderately high inflammation reaction, the inflammation reaction of the submucosa was slight with both sutures remaining unabsorbed. Infiltration of inflammatory cells was found within the suture interstices (Fig. 6).
Immune response to nylon sutures
Infiltration of various inflammatory cells was examined from the tissues surrounding the sutures. While polymorphonuclear leukocytes (PMNL) were mainly observed during the early stage, the proportion of macrophages present compared to other cell types increased as time proceeded. Although infiltration of inflammatory cells, such as PMNL, neutrophils, and macrophages, could be observed around the suture, infiltration within the connective tissue was low. As for nylon suture located on the keratinized gingiva, seven days after suturing the number of PMNLs, lymphocytes, and macrophages decreased, from the surrounding tissue of the suture toward the submucosa tissue (Fig. 7). Fourteen days post-suturing, the infiltration of inflammatory cells was not significant. In particular, the infiltration of inflammatory cells within the connective tissue was very rare (Figs. 8 and 9). The difference in inflammation reaction between the keratinized gingiva and the buccal mucosa was not significant. Moreover, there was no difference in the inflammation reaction between the tissues surrounding the suture as time proceeded.
Statistical analysis
The inflammatory reaction grade was more severe in the buccal mucosa than keratinized gingiva in all groups, but there was no statistical significance (Table 1). The inflammatory reaction grade according to the point in time showed that lymphocyte and macrophage infiltration were significantly low in the keratinized gingiva after three days, whereas macrophage infiltration was significantly high in the buccal mucosa after one week (Table 2).
DISCUSSION
Adaptation and maintenance of the wound site by sutures are critical events for the success of a surgical procedure. However, the existence of foreign material within the wound can increase the susceptibility to tissue infection [17]. Infection caused by the incision of a wound site, spread of infection during suturing and suture removal, and the delay of healing after surgery can all lead to a serious situation for a patient with a chronic disease, such as diabetes mellitus or cardiovascular disease. It has been reported that the risk of infection is increased by the presence of a suture within a wound [18].
Therefore, the importance of yielding the minimum immune response, which is an ideal result of suturing, should be considered with great attention when selecting suture type. Accordingly, this study was conducted to compare and evaluate the function of three suture types, all of which are widely used in intraoral surgeries, through the comparison of their tissue affinities. One of the most important functions of a suture is to maintain the stability of the wound edges until they can sustain themselves. The removal of oral surgery sutures is routinely performed one week post-surgery. However, in the case of regeneration therapy, maintenance of the suture for at least two weeks is frequently allowed in clinical practice for the enhancement of tissue maturity [19].
Therefore, in this study, a long term evaluation was used to examine the early- and late-stage immune responses. The experiment was divided into three time periods for the observation of acute inflammation, the common period of suture removal, and the maximum tensile force of the incision: three days post suturing, seven days post suturing, and 14 days post suturing. As for the sutures in the experiment, silk, polyglycolic acid, and nylon sutures were selected based on their wide utilization in clinical practice.
According to the study by Cardaropoli et al. [20] healing of the soft tissue in the extraction site included highly organized fibrous connective tissues at 30 days post-extraction, while the isolation of the newly formed hard tissue was mainly composed of woven bone and marginal mucosa at 60 days post-extraction. In this study, the suturing was conducted two months after the extraction to rule out the influence of the immune response caused by the soft tissue healing process and the woven bone formation.
The keratinized gingiva of the mandibular premolar regions and the buccal mucosa of the maxillary premolar regions were selected as the suture application sites for this study. Castelli et al. [15] reported that the mucosa is susceptible to the infiltration of inflammatory cells due to its composition of muscle fibers, minor saliva glands, and common connective tissues. Romanos et al. [21] immunohistologically identified type V collagen as containing the largest portion of lamina propria in sound keratinized gingiva. They also showed that type V collagen has great resistance to collagenase and acts as a mechanical barrier to bacterial penetration. It was also shown in this study that the sutures located on the buccal mucosa resulted in a higher infiltration of inflammatory cells into the internal tissue of the sutures than did those on the keratinized gingiva. However, the difference in the inflammation reaction between suture locations at 14 days post-suturing was insignificant.
The keratinized gingiva of the mandibular premolar regions and the buccal mucosa of the maxillary premolar regions were selected as the suture application sites for this study. Castelli et al. [15] reported that the mucosa is susceptible to the infiltration of inflammatory cells due to its composition of muscle fibers, minor saliva glands, and common connective tissues. Romanos et al. [21] immunohistologically identified type V collagen as containing the largest portion of lamina propria in sound keratinized gingiva. They also showed that type V collagen has great resistance to collagenase and acts as a mechanical barrier to bacterial penetration. It was also shown in this study that the sutures located on the buccal mucosa resulted in a higher infiltration of inflammatory cells into the internal tissue of the sutures than did those on the keratinized gingiva. However, the difference in the inflammation reaction between suture locations at 14 days post-suturing was insignificant.
In addition, it has been suggested that the physical form of a suture determines the degree of the inflammation reaction [15]. In many studies, the cause of the severe inflammation reaction observed in multifilament sutures, compared with monofilament sutures, has been referred to as 'the wicking effect' and results in the spread of the infection among the multifilament sutures and the presence of bacteria within the suture interstices [8,12,22]. However, Grigg et al. [4] found that silk did not produce more fluid movement by capillary action than coated Vicryl, and produced less than a polymer suture. According to a clinical study on the influence of suture absorption in two types of multifilament sutures and the resulting complication occurrence of wound healing and the failure of dental implants by Ivanoff and Windmark, neither type of suture showed any infection or implant failure [5]. Sortino et al. [23] counted the number of microorganisms with a light microscope in order to evaluate the inflammation reactions after removal of silk and polymer sutures from an intraoral environment eight days post-suturing. They reported that there was no significant difference between the treatment outcomes with regard to suture type, due to similar distributions of aerobic and anaerobic bacteria within the sutures. Also, it was reported that comparisons of infection, dehiscence, redness, scar hyperplasia, and patient satisfaction between nylon and polymer sutures from a skin biopsy at two weeks and six months after suturing did not show any significant differences [24]. In our study, blood clots from the trauma of suturing and infiltration of inflammatory cells around the suture and within the connective tissue due to acute inflammation reaction were observed around the suture and within the submucosa during the entire period of observation. However, there were no significant differences in the degree of inflammation among the three types of suture located on the keratinized gingiva. As for the silk and polyglycolic acid sutures, the existence of neutrophils within suture interstices and the migration of leukocytes were identified throughout the study.
In this study, intramuscular injection was administered with 2 mL of gentamicin for three days after suturing, and plaque control was performed with normal saline and 2% chlorhexidine. According to the study of Leknes et al. [25] on immune responses due to the use of silk and expanded polytetrafluoroethylene sutured onto the mandibular keratinized gingiva of a beagle, the administration of 2% chlorhexidine and systemic broad-spectrum antibiotics reduced the formation of biofilm and inflammation within the suture path. On the other hand, it was reported that the use of chlorhexidine had no effect on the species or existence of microorganisms, regardless of the kind of suture utilized [23]. However, because it used human participants, the latter study was considered to be incapable of strict control. Moreover, considering that the surgery sites were at the mandibular right angle area, the maintenance of oral hygiene was regarded as unmanageable. In this study, post suturing oral disinfection was conducted daily with 2% chlorhexidine, and unlike the study of Sortino et al. [23], the oral hygiene control of the suture sites in the mandibular premolar region (P1-P4) was possible, resulting in a definite outcome.
In conclusion, the nylon monofilament suture resulted in a favorable treatment outcome when placed in the alveolar mucosa, lesions arising from acute inflammation or an environment in which oral hygiene maintenance was unavailable. On the other hand, the structural difference in the monofilament and the multifilament sutures, with regard to immune response, did not affect the treatment outcome when placed in histologically dense keratinized gingiva with good oral hygiene.





 XML Download
XML Download