

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Aggressive periodontitis is characterized by a rapid loss of clinical attachment and alveolar bone and normally affects young adults [1-3]. As opposed to chronic periodontitis, the amount of biofilm and calculus accumulation in aggressive periodontitis subjects is inconsistent with the severity and progression of the periodontal destruction. These infections are subdivided into localized and generalized cases, according to the extent of the periodontal destruction [4]. Diagnosis of aggressive periodontitis requires exclusion of the presence of systemic diseases that may severely impair host defenses and lead to premature tooth loss [2].
A review of the published literature suggests that the prevalence of aggressive periodontitis may vary significantly among countries and ethnicities. Low prevalence rates ranging between 0.1% and 0.2% have been reported in Europe [5-7], whereas high prevalence rates ranging between 3% and 10% have been reported in Brazil [8,9], Iraq [10], Indonesia [11], and the United States [1].
There are some reports that the prevalence of aggressive periodontitis differs by gender. Baer [12] reported that chronic periodontitis is common in men, but aggressive periodontitis is common in women, and Hørmand and Frandsen [13] reported that the difference according to gender decreases with advancing ages. A recent survey among Ugandan students aged 12 to 25 years found that aggressive periodontitis was more prevalent in males [14].
Many reports have discussed host susceptibility factors for aggressive periodontitis, including family aggregation, single nucleotide polymorphisms, polymorphonuclear neutrophils, antibodies to bacteria, smoking, stress, a local contributing factor (root morphology), and herpes virus infections [15]. Schenkein et al. [16] reported that smoking, as assessed by serum cotinine concentrations, has a significant effect on the extent and severity of periodontal attachment loss in patients with generalized early onset periodontitis. It has been demonstrated that there are differences in the oxygen saturation of hemoglobin in the gingiva of smokers and nonsmokers, suggesting that smokers have functional impairments in the gingival microcirculation [17].
It is easy to miss proper cure time without early detection of disease and teeth are especially likely to be lost as a result of progression of aggressive periodontitis [18]. Even though there have been attempts to analyze aggressive periodontitis biochemically and microbiologically, there is no specific way to discover aggressive periodontitis early [1]. Currently, early detection depends primarily on clinical and radiographic examination methods [1]. However, there are few epidemiologic studies about aggressive periodontitis of Koreans. The epidemiologic studies of disease prevalence and other clinical characteristics are invaluable in providing proper treatment.
The aim of this study was to assess the prevalence of aggressive periodontitis and to measure the extent of periodontal breakdown of those patients who visited Wonkwang Daejeon Dental Hospital.
MATERIALS AND METHODS
Subjects
We conducted a survey of the 1,692 patients who visited the Department of Periodontology, Wonkwang Daejeon Dental Hospital for the first time from January to December, 2010. The subjects of this study consisted of 1,020 males (60.3%) and 672 females (39.7%). We diagnosed patients with aggressive periodontitis according to the criteria of the American Academy of Periodontology International Classification of 1999 (Table 1). Additional inclusion criteria were as follows: 1) The patient's was under 40 years old, 2) The patients had familial aggregation of periodontal disease.
All patients were thoroughly informed about the procedure and gave written consent for inclusion in the study. This study was approved by the Institutional Review Board of Wonkwang University Dental Hospital (IRB number WKD IRB 20110201).
Clinical examinations
Complete medical and dental histories, including familial aggregation of periodontal disease and smoking habits, were taken before clinical periodontal assessment.
All clinical assessments and examinations including probing depths, gingival recession, and bleeding on probing at six points per tooth, were carried out by a single examiner. The probing pocket depth was measured from the free gingiva to the pocket base by using a periodontal probe (PW, Hu Friedy Manufacturing Co., Chicago, IL, USA). We measured the gingival recession from the cement enamel junction to the free gingiva with the same tool. We determined the clinical attachment loss, which is the length from the cement enamel junction to the depth of the pocket base, as the sum total of the depth of the pocket and gingival recession. Gross deposits of dental calculus and plaque obstructing the cemento-enamel junction were removed prior to these measurements. All fully erupted permanent teeth were examined, excluding the third molars. After the clinical examination, we took periapical radiographs of the full mouth and analyzed the bone level and any root deformity or missing teeth using PiView STAR software (Infinitt Co., Seoul, Korea; data not shown).
Statistical analysis
Data management procedures were carried out with SPSS ver. 14.0 (SPSS Inc., Chicago, IL, USA). An independent t-test and, one way analysis of variance with Turkey honestly significant difference post hoc test were used to analyze the difference in pocket depth, gingival recession, periodontal attachment loss, and tooth mortality of representative teeth. A P-value <0.05 was considered significant.
RESULTS
The survey subjects were 1,692 people including 1,020 males and 672 females. Twenty-eight of the 1,692 patients were diagnosed with aggressive periodontitis, and the prevalence of morbidity was 1.65%. The generalized form was more common than the localized form by a ratio of 27:1. The average age was 34.46, and the sex ratio was 1.65:1 (male:female). The number of males with aggressive periodontitis was significantly higher than that of females. However, given the sex ratio of the population, there was no statistically significant difference by gender (P>0.05) (Table 2).
Nine (32.14%) of 28 aggressive periodontitis patients were present smokers, and 7 more had a smoking history; together, they were over half of the cases (57.14%) (Table 3).
The probing pocket depth of the maxillary first molar was deeper than that of the other teeth (P<0.001). However, there was no statistically significant difference between the maxillary and mandibular first molar (P=0.42). The probing pocket depth of the maxillary first premolar was significantly deeper than that of the mandibular first premolar (P=0.045) (Table 4).
Gingival recession was the most serious at the maxillary first molar. Within comparing the opposing dentition, the gingival recession of the maxillary teeth was significantly greater than that of the mandibular teeth, except at the central incisor (Table 5).
The attachment loss was higher at the maxillary first molar than at the other teeth. The attachment loss of the first premolar and first molar was significantly higher in the maxilla than in the mandible (Table 6).
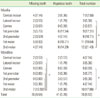
The distribution of the missing teeth due to periodontal disease was recorded. All teeth missing due to congenital reasons, orthodontic treatment, caries, or trauma, were excluded from the distribution analysis. The average number of missing teeth was 1.29 at the first visit, but if we include the teeth that were diagnosed as hopeless those found to be floating, it doubled to 2.75. The mandibular second molar showed the highest tooth mortality from mandible group, and this finding was statistically significant (P<0.05). However, there was no statistically significant difference between the maxillary second molar and mandibular second molar (P=0.176). The result was same when hopeless teeth were included: second molars were the most commonly missing teeth followed by the first molars. In addition, most of the canines were preserved in most patients (Tables 7, 8).
DISCUSSION
In this study, we assessed the prevalence and periodontal clinical parameters of the aggressive periodontitis patients who visited the Wonkwang University Daejeon Dental Hospital for periodontal treatment.
Only a few large scale surveys of aggressive periodontitis have been conducted globally. Albandar et al. [1] reported that the prevalence of aggressive periodontitis was 10% in African-American, 5% in Hispanic and 1.3% in white United State adolescents between 13 and 17 years of age. Harley and Floyd [19] reported a prevalence of 0.8% among Nigerian teenagers. The prevalence of schoolchildren with aggressive periodontitis in Iraq was 1.8% [20]. Kowashi [21] reported that the prevalence of aggressive periodontitis was 0.47% in 19 to 28-year-olds in Japan. The prevalence was 1.65% in the present study, which limited the patients' to those under 40 years old. This result is notably different from the findings of other studies, but due to some differences in sampling, study design, classification of disease, and standards of analysis, the results are not necessarily comparable to other studies. The average age was 34.46, which was somewhat higher than of previous clinical studies. It seems that this is because the research subjects were patients who presented to the hospital due to feelings of discomfort from the progressing disease rather than youth without symptoms. Few epidemiologic studies have gathered information on clinical features and degree of periodontal destruction of aggressive periodontitis patients in Korea. Further epidemiologic studies of larger populations are needed to assess the exact prevalence of aggressive periodontitis and gather basic data to assist in developing proper treatment.
Some epidemiological studies have shown that the prevalence of periodontal disease is often higher among young females. Baer [12] estimated that the female/male ratio was about 3:1, suggesting that females are 3 times more likely to develop the disease than males. Hørmand and Frandsen [13] examined a large group comprising 156 aggressive periodontitis patients ranging in age from 12 to 32 years and concluded that the disease affects females more often than males with a ratio of 2.5:1. In the present study, however, it was shown that the number of males affected with aggressive periodontitis was higher than that of females (2.5:1), which differs from the results of these previous studies. However, in light of the gender ratio (1.47:1) of the study population, there was no statistically significant difference in prevalence by gender (P>0.05). More studies are required to determine the gender ratio in aggressive periodontitis prevalence in Koreans.
Over the half of the aggressive periodontitis patients (57.14%) in this study had a smoking history. This agrees with a previous study finding that there is a relation between aggressive periodontitis and smoking. Schenkein et al. [16] revealed that 20% of localized aggressive periodontitis patients and 43% of generalized aggressive periodontitis patients were smokers, and it is sometimes higher than smoking rate of people who are periodontally healthy (16%). It is unclear whether there is a consistent effect of smoking on the bacterial population selection. However, smokers should be encouraged by their dentists or treating physicians to cease smoking, emphasizing that smoking can increase the risk of periodontal diseases.
In the current study, serious attachment loss over 5 mm was observed at the first molar. It is assumed that this is because the first molars are affected earlier by localized aggressive periodontitis. In localized aggressive periodontitis the only teeth affected are the first molars and incisors. Although there are cases in which aggressive periodontitis has been arrested for some time after periodontal therapy, aggressive periodontitis develops as localized disease and then may progress into a generalized form with the involvement of more teeth with advancing age [13]. Most of the subjects in this study had the generalized form; thus the first molar may have suffered more attachment loss.
Kim et al. [22] reported that the average number of missing teeth in Korean adults aged 30 to 34 years was 1.24. In this study, the average number of missing teeth was 1.29 at the first visit, but if we include the teeth diagnosed as hopeless, it doubled to 2.75. Considering the subjects' age was limited to under 40 years, this was slightly higher than the results of previous studies. We can assume that this result was affected by the aggressive periodontitis type, as the generalized form was more common at a ratio of 27:1 in this study. Tooth loss can be a natural consequence of the advance of periodontitis [23-25]. More specifically, tooth loss parallels clinical attachment loss, which is a measure of disease severity [26]. The most frequently missing teeth in current study were second molars (19.64%), followed by first molars (14.29%). Ng et al. [27] reported that the provision of periodontal maintenance led to minimal tooth loss, especially due to periodontitis, for a mean period of 10 years after active periodontal therapy. Therefore, we can assume that the high percentage of second molar tooth loss might be because the second molar had additional susceptibility factors such as occlusal interference, hygienic difficulty, root cracks, and so on.
Considering the small population of this study, its findings should be confirmed by large scale, methodologically sophisticated studies. Within the limitations of this study, it was shown that the periodontal breakdown evaluated by attachment loss was the highest at the first molars and most of the aggressive periodontitis patients had their periodontal health impaired without early detection of their disease. Early detection may facilitate the successful management of aggressive periodontitis. Therefore, periodontologists should inform patients of the presence of aggressive periodontitis characterized by rapid attachment loss and bone destruction, early onset, and the difference between aggressive periodontitis and chronic periodontitis. They should also encourage younger patients to get regular periodontal check ups and treatment. Further epidemiologic, clinical, and genetically based studies for providing exact diagnosis and treatment of aggressive periodontitis will be needed.







 XML Download
XML Download