

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The purposes of soft tissue management around dental implants are successful primary closure, papillary reconstruction, gain of keratinized tissue and preservation of ridge contour. Keratinized tissue is a specialized mucosa covered with keratin or parakeratin which includes the free and attached gingiva and extends from the gingival margin to the mucogingival junction. However, The need and significance of keratinized tissue around dental implants is a controversial issue. Wennstrom et al. [1] reported that there is no clinical difference between teeth with and without adequate keratinized tissue and no association between the width of keratinized tissue and the presence of bleeding on probing. Bengazi et al. [2] reported that the width of keratinized tissue was a poor predictor for occurrence of soft tissue recession. The recession was primarily the result of a remodeling of the soft tissue for establishing appropriate biological dimensions. Albrektsson et al. [3] reported that dental implants may have a high survival rate, irrespective of keratinized conditions. Although the significance of keratinized tissue is still controversial, it is certain that the attached gingiva provides increased resistance of the periodontium to external injury, contributes to the stabilization of the gingival margin position, and aids in the dissipation of physiological forces that are exerted by the muscular fibers of the alveolar mucosa on the gingival tissues [4]. Despite the observation that the lack of keratinized tissue does not influence long term implant survival, the preservation and the reconstruction of keratinized tissue around dental implants could be important. Many surgical techniques have been utilized to augment gingival tissue dimensions. Langer and Sullivan [5] suggested techniques to obtain adequate amounts of keratinized tissue around two stage implants, primarily based on the preservation of keratinized tissue over the edentulous ridge. At the time of implant exposure, apically positioned or laterally positioned flaps were proposed to reconstruct keratinized tissue of adequate width around implants. When the amount of keratinized tissue over the edentulous ridge was minimal, a free gingival graft (FGG) was suggested. These techniques however are associated with significant patient morbidity due to the need for creating a wound at the palatal donor site. Recently, many of the disadvantages of the classic procedure have been overcome by modification and the use of tissue engineering materials. Wei et al. [6] used an acellular dermal matrix allograft to achieve increased attached gingiva. Simion [7] used a collagen membrane for soft tissue healing. More recently, a collagen matrix has been proposed as a substitute for the palatal donor tissue to augment gingival tissue dimensions [8]. Here we performed APF only, APF combined with FGG, and APF combined with collagen matrix coverage at the second implant surgery and evaluated the width of keratinized tissue around dental implant.
CASE DESCRIPTION
Subjects
Nine patients were selected from those who had received treatments at the Department of Periodontics, Chosun University Dental Hospital, Gwangju, Korea. The inclusion criteria were as follows:
All patients received the ethics committee approved informed consent form. This study protocol was approved by the Chosun University Dental Hospital Institutional Review Board (CDMDIRB-0902-14).
Surgical procedure
We performed APF, APF combined with FGG, and APF combined with collagen matrix coverage (Collatape®, Zimmer Dental, Carlsbad, USA) at the second implant surgery. The time point soft tissue management was 4 months after the initial implant surgery. For a proper standardization between baseline and follow up data, periodontal probes were used to measure keratinized tissue. The measurements were taken vertically from the gingival crest level.
Three different surgical techniques were performed on nine patients. The surgical techniques were determined based on the following criteria:
If the keratinized tissue had a width greater than three millimeters, the APF technique was performed.
If the keratinized tissue width was in the two to three-millimeter range, the APF combined with collagen matrix coverage technique was performed.
If the keratinized tissue was minimal, then the APF combined with FGG technique was performed.
At the time of the surgery, local anesthesia was administered and the surgical procedure was performed. After patient selection was complete, all of the cases underwent a surgical procedure designed to enlarge the area of keratinized tissue. The surgical technique used for the groups consisted of the following steps:
Case 1 - Apically positioned flap
Using a #15C blade (Ace Surgical Supply Co., Brockton, USA), a mucosal partial-thickness flap was raised. The recipient site was prepared by sharp dissection in order to create a periosteal bed free of any muscle attachment. The resulting flap was sutured at the base of the newly created vestibule with 5-0 non-resorbable nylon sutures (Happylon, Shirakawa Co., Takayama, Japan) (Fig. 1).
Case 2 - APF combined with FGG
FGGs were performed according to the original technique described by Sullivan and Atkins. A recipient bed was prepared similar to Case 1 and a free graft was harvested from the palate (Fig. 2).
Case 3 - APF combined with collagen matrix coverage
After preparing the recipient site, collagen matrix was trimmed and shaped to fit the recipient site. Collagen matrix was fixed the same manner as in the FGG method (Fig. 3). All three patient cases were then instructed to rinse twice daily with a chlorhexidine mouth rinse (0.12%) for 2 weeks. Anti-inflammatory therapy (Amoxicillin 625 mg) was prescribed, and the patients were given instructions to take this drug for three days. Sutures were removed after 10 days. The collagen matrices used in this clinical evaluation were Collatape® (Zimmer Dental, Carlsbad, USA) in sterile, individual bubble packs. These matrices are fabricated using collagen obtained from bovine deep flexor (Achilles) tendon, and function to control bleeding, stabilize blood clots, protect wound beds, and provide a matrix for tissue ingrowth, and they absorb in approximately 10-14 days. However, if exposed directly to the oral environment, they will be absorbed more rapidly. To test the toxicity of Collatape® (Zimmer Dental, Carlsbad, USA), Luitaud et al. [9] seeded epithelial cells onto the CollaTape, and epithelium formation was analyzed at set times. The epithelial cells adhered, proliferated, and began to stratify as early as 2 days post-seeding. Advanced stratification was observed at 6 days post-seeding. This result confirms that Collatape® (Zimmer Dental, Carlsbad, USA) material is nontoxic and capable of supporting fibroblast adhesion and growth.
Clinical measurements
Clinical evaluation of keratinized gingival was performed by measuring the distance from the gingival crest to the mucogingival junction at the mid-buccal point, using a periodontal probe (PCP 10®, Hu-Friedy, Chicago, USA). It was recorded pre-operatively and after soft tissue healing.
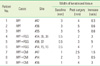
The subject consisted of 9 patients; 3 subjects were allocated in the APF case, 3 subjects were allocated in the APF combined with FGG, and 3 subjects were allocated in the APF combined with collagen matrix coverage. No patients in any of the cases developed any significant complications. The change of keratinized tissue width is shown in Table 1. The increased ratio was 0.3, 0.6, and 0.6 for the three subjects in the APF cases 3, 5, and 7 for the three subjects in the APF combined with FGG cases, and 1.5, 0.5, and 3 for the three subjects in the APF combined with collagen matrix coverage cases. These results showed greatest increase in the keratinized tissue for the FGG cases, and a mild to moderate increase for the APF and APF combined with collagen matrix coverage case. At baseline, the width of the keratinized tissue in the FGG cases were minimal and the other cases showed a similar width, which ranged from 1 to 3 mm. The amount of the keratinized tissue increased over the 3 to 4-week post-surgical period in all three cases. The APF combined with collagen matrix coverage cases show a similar or greater increase of keratinized tissue increase as in APF only areas. Similarly to the APF combined with FGG areas, the APF combined with collagen matrix coverage cases showed more favorable physiologic morphology then the APF only cases.
DISCUSSION
The controversy regarding the need for an 'adequate' width of keratinized tissue around teeth in order to preserve periodontal health still exists. There are clinical situations where the presence of a certain width of keratinized tissue may be important in maintaining periodontal health and preventing soft tissue recession, such as in the areas around fixed prosthetic restorations [10]. In spite of the observation that the lack of keratinized tissue may not influence implant survival, the careful management of soft tissue around implants is considered essential by clinicians [11-15]. The increase of keratinized tissue has been achieved traditionally using the FGG [16]. Augmentation of keratinized tissue width and vestibular deepening with autogenous FGGs has been reported to be a predictable and effective method [17-19].
Although the incidence of complications is very low, discomfort and pain at the donor site are frequently observed. This technique causes other wounds at the palatal site, and increases the morbidity of the patient.
To avoid this morbidity, a substitute for palatal donor tissue has been studied. For example, acellular dermal matrix allograft, collagen membrane, and collagen matrix have been used, instead of palatal tissue. The acellular dermal matrix allograft showed good results at soft tissue augmentation, because this material is derived from human cadavers, however, it is associated with ethical concerns and the possible risk of disease transmission [20-22].
Collagen membrane has also been shown to have a positive effect on soft tissue augmentation and healing, but collagen matrix has a more porous layer meaning greater keratinized tissue can be achieved because of the space creating effect and blood clot formation [23]. Thus, the collagen matrix can be expected to be more effective at augmenting keratinized tissue. The main objective of this clinical study was to evaluate the changes in width of keratinized tissue following three surgical techniques, APF, APF combined with FGG, and APF combined with collagen matrix coverage. The result from this clinical study indicated that after 3-4 weeks, all of the cases achieved keratinized tissue. Furthermore, after 3-4 weeks, the three cases also achieved proliferation and maturation. The FGG cases showed a greater increase of keratinized tissue, and the APF combined with collagen matrix coverage cases showed more keratinized tissue increase than the APF only cases. The keratinized tissue after surgery in the APF combined with collagen matrix coverage cases were characterized by more physiologic and favorable morphology than the APF only cases. It is believed that the collagen matrix acts as a scaffold to prevent the mucosal relapse, and protection of the recipient bed.
Evidence of the advantages of collagen matrix is insufficient. Therefore, further studies are necessary to determine the influence of collagen matrix on the recipient bed, and on how to prolong the short absorption period of collagen matrix (10-14 days).



 XML Download
XML Download