

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Today, endosseous dental implants are an established treatment alternative for edentulous and partial edentulous patients. Various surface characteristics ranging from relatively smooth machined surfaces to more roughened surfaces are available and survival rate of implant is increased [1]. However, as better results and higher success rate have been reported annually, implant-related complications have been also increasing.
The term peri-implant disease is collectively used to describe biological complication in implant dentistry, including periimplant mucositis and peri-implantitis. While peri-implant mucositis includes reversible inflammatory reactions located solely in the mucosa adjacent to an implant, peri-implantitis was defined as an inflammatory process that affects all tissues around an osseointegrated implant in function resulting in a loss of the supporting alveolar bone. Diagnosis of peri-implant infections is based on peri-implant probing depth, evaluation of peri-implant keratinized mucosa, presence of bleeding on probing and suppuration, radiographic evaluation, evaluation of implant mobility, and analysis of peri-implant sulcus fluid [2].
The main etiological factor of peri-implant diseases is the accumulation of dental plaque that shows a very similar composition if compared to bacterial biofilms found in periodontal pockets [3-5]. These bacteria present on implant surfaces may lead to an inflammation spreads apically and results in bone loss. Peri-implant tissues are easily susceptible to any bacteria or mechanical attack because a supracrestal connective area that is highly acellular and with a great number of collagen fibers [6]. Therefore, the removal of bacterial biofilms seems to be a prerequisite in the therapy of peri-implantitis especially when a regenerative procedure is planned [7-9].
In recent years, several treatment strategies (i.e., mechanical, chemical) have been proposed for the treatment of peri-implant infection [10]. Mechanical debridement is usually performed using plastic curettes or rubber cups [11-13]. But mechanical methods alone have been proven to be insufficient in the elimination of bacteria on roughened implant surfaces [11]. Although air powder flow was also successfully used for implant surface decontamination in vitro, there are limitations in the application because it can lead to microscopically visible alterations of the implant surface and be associated with an increased risk of emphysema [13-15]. Chemical methods with citric acid, chlorhexidine gluconate, hydrogen peroxide, tetracycline chloridrate, stannous fluoride were suggested even if they leave microscopic residues or resulted in a loss of implant surface roughness when viewed on scanning electron microscopy [10,16,17].
Nowadays, laser is widely used in dentistry and many authors suggested its use for treatment of peri-implant infections. Various advantageous characteristics, such as easy handling, hemostatic effects and bactericidal effects against periodontopathic pathogens have been suggested to improve treatment outcomes. However, several potential risks complicate their clinical use. The neodymium-doped: yttrium-aluminum-garnet (Nd:YAG) laser is not suitable for implant therapy since it easily ablates titanium irrespective of output energy [18,19]. Only the CO2 laser, the diode laser, and the erbium:yttrium-aluminium-garnet (Er:YAG) laser may be suitable for the irradiation of titanium surfaces because the implant body temperature did not increase significantly during its application. But neither CO2 nor diode lasers were effective in removing plaque biofilms from titanium implants [20-23]. On the other hand, Er:YAG laser, emitting at a wavelength of 2.94 µm, seemed to be capable of effectively removing plaque and calculus from both smooth and rough implant surfaces without injuring their surfaces [24-27].
In the earlier studies, the effects of Er:YAG laser on the different kinds of implant surfaces have been evaluated to find the most ideal laser application conditions, and this study was performed on that extension. The purpose of this study was to evaluate the effect of Er:YAG laser irradiation on the microstructural change of hydroxyapatite (HA)-coated implant surface according to the laser energy and the application time.
MATERIALS AND METHODS
Implants
Ten HA-coated implants (SCREW-VENT, Zimmer Dental Inc., Carlsbad, CA, USA) of a diameter of 4.7 mm and a length of 16 mm were used in this study. One was the control group and the others were the test group.
Laser apparatus
The applied laser system was an Er:YAG laser (KEY3, KaVo, Biberach, German) emitting pulsed infrared radiation at an wavelength of 2.94 µm with a truncated cone tip. Er:YAG laser has variable pulse frequency (1-15 pps) and pulse energy (60-260 mJ).
Surface evaluation
To evaluate the implant surface topography qualitatively, we used scanning electron microscope (SEM; S-2300, Hitachi, Tokyo, Japan). And mechanical contact profilometer (Form Talysurf Laser 635, Taylor Hobson, Leicester, UK) with a contact stylus instrument made of diamond was used to present roughness data in the form of numeric standard roughness parameters.
Specimen assignment
The control group didn't have laser irradiation and the test group was irradiated with the different energy and time conditions. Test group was divided into 3 subgroups (group I, II, III) by laser application energy (100, 140, and 180 mJ/pulse). Three different irradiation time (1, 1.5, and 2 minutes) was applied on each subgroups.
Surface roughness measurement before laser application
At first, implant container was made using impression putty so as to fix the implant in position. After the measurement point had been marked by water-proof maker pen on the container, implant surface roughness was measured three times each on the 3rd, 8th, and 13th valley by mechanical contact profilometer. With a profilometer, the average roughness (Ra), one of the height-descriptive two-dimensional parameters profiles was measured and recorded with a diamond-tipped stylus of 5 µm radius running horizontally to the long axis of the implant.
Laser application and surface roughness re-measurement
Nine implants were assigned to 3 test groups, three implants per one group. Laser on the setting of 100 mJ/pulse, 10 Hz was irradiated on the three implants of group I during 1 minute, 1.5 minutes and 2 minutes each. In the same time protocol, energy of 140 mJ/pulse was irradiated to group II and 180 mJ/pulse, 10 Hz to group III. Each laser irradiation area was 2×2 mm2 on the 2nd-4th, 7th-9th, and 12th-14th valleys of the implant. The laser beam was irradiated under water irrigation and the fiber tips were guided parallel to the implant surface in near contact mode which allows the working distance between the tip of the laser and the exposed surface to be approximately 0.5 mm. The angle between the fiber tips and implant surface was 90 degree and the laser handpiece was moved along the horizontal, vertical and oblique pathways repeatedly to provide even laser exposure to the surface. The laser-irradiated implants were dehydrated and surface roughness was re-measured on the same area.
SEM observation
The specimens were sputter-coated with a thin layer of gold for 10 minutes and examined using SEM with magnification of 500 and 2,000. By examining the SEM images, the changes of implant surface were evaluated.
Statistical analysis
A software package was used for the statistical analysis (SPSS 17.0, SPSS Inc., Chicago, IL, USA). Mean values and standard deviations were then calculated for the implant surface roughness. Group comparison was performed by the Wilcoxon's signed rank sum test and differences between before and after the laser irradiation were considered to be significant when P<0.05.
RESULTS
SEM evaluation
Control group
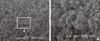
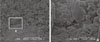
One HA-coating implant that didn't have any surface treatment was evaluated using SEM with magnification of 500 and 2,000. It showed irregular rough surface with various sized crystalline HA (Fig. 1).
Test groups
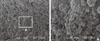
In group I (100 mJ/pulse), there was no remarkable surface change on condition of 1 minute (Fig. 2). But on condition of 1.5 and 2 minutes, surface melting and cracks were observed on magnification of 2,000. In addition, surface was partially flattened (Figs. 3 and 4).
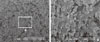
Group II (140 mJ/pulse) showed more significant change than group I and was shown a severe surface melting and peeling of HA particles. In addition, the surface had deep and wide cracks (Figs. 5, 6, 7).
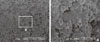
In the group III (180 mJ/pulse), surface melting and peeling area of HA particles were observed wider and deeper than group II. As a result of this, there was a tendency showing that the surface roughness had been gradually reduced. This tendency was more significant with increased irradiation time (Figs. 8, 9, 10).
Surface roughness measurement
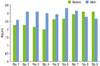
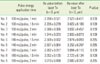
The mean surface roughness of pretreatment 9 specimens was 2.507±0.352 µm. The amount of change between before and after the laser irradiation was each 0.319, 0.817, 0.945, 0.989, 0.302, 0.645, 0.212, -0.329 and -0.414 µm respectively from No. 1 to No. 9. The average roughness values were increased in all group I and II, irrespective of the irradiation energy and time. But in group III, while the roughness value was increased at 1 minute, it was decreased at 1.5 and 2 minutes. But this all changes were not statistically significant (P>0.05) (Table 1, Fig. 11).
DISCUSSION
This study was evaluated the effect of Er:YAG laser irradiation on the microstructural change of HA-coated implant surface according to the laser energy and the application time. While HA-coated implant surface showed no significant change by Er:YAG laser irradiation under experimental condition of 100 mJ/pulse, 1 minute, surface melting and cracks were founded on condition of 100 mJ/pulse, 1.5 and 2 minutes. 140 mJ/pulse and 180 mJ/pulse group had surface melting and peeling area of HA particles. But in all experimental groups, the roughness value change was not statistically significant.
The main etiological factor of peri-implant diseases is the accumulation of dental plaque. Therefore it is essential to remove the dental plaque and decontaminate implant surface for treatment of peri-implant disease. To achieve this, many mechanical and chemical methods were developed but nothing was satisfactory [10-17,28,29]. Nowadays, laser is widely used in dentistry. Especially Er:YAG laser possesses bactericidal decontamination effectiveness and seemed to be capable of effectively removing plaque and calculus without injuring titanium surfaces and adjacent bone [27,30]. And Er:YAG laser was showed biocompatibility more than ultrasonic scaler on implant surface [26]. Therefore Er:YAG laser was used in this study. Kreisler et al. [19] demonstrated that titanium plasma sprayed, sandblasted and acid-etched, HA-coated and machine-polished surface were influenced by the Er:YAG laser and the power output must be limited to avoid surface damage. Therefore the respective surface determined the energy necessary to induce surface alterations. Also the working angle, application mode, time and water cooling influenced on surface alterations.
In this study, HA-coated implant produced by a plasma-spraying technique on pure titanium is used [31]. It was rough surface between 2.0-3.0 µm in (Sa) value and Albrektsson and Wennerberg [32] and Cook [33] suggested that it was supposed to promote osseointegration in contrast to a pure titanium surface. But it was a much greater affinity of lipopolysaccharides (LPS) than pure titanium and the risk of increased peri-implantitis because of high charged surface [9,34]. And HA-coated implant surface was damaged by metal curet, plastic curet, ultrasonic scaler and air powder flow [13].
Kreisler et al. [27,30] reported mean bacterial reductions of 98% and no excessive temperature elevations at pulse energy of 60 and 120 mJ and a 10 Hz. And Schwarz et al. [26] reported no significant alteration of HA-coated implant surface at pulse energy of 100 mJ, 10 Hz and 2 minutes. Overall the test group I is irradiated pulse energy of 100 mJ and 10 Hz that is effective detoxification and no significant surface alteration.
The angle of the application tip is another important factor for decreasing root substance removal. Folwaczny et al. [35] reported that the angle of the application tip to the root surface has a strong influence on the amount of root substance removed during Er:YAG laser irradiation and the effect is maximum at an angle of 90 degrees. In this study for maximum energy application, the irradiation angle was 90 degrees and the distance from the implant surface was 0.5 mm.
The laser beam was irradiated under maximum water irrigation to minimize thermal influence. Eriksson and Albrektsson [36] reported that a temperature threshold levels for heat-induced bone tissue injury is 47℃. The use of water coolant minimizes heat generation by cooling the irradiated area and absorbing excessive laser energy. In addition, a water spray facilitates hard tissue ablation by keeping the target moist [37,38].
In this study, local areas with surface melting and cracks were founded at 100 mJ/pulse, 1.5 minutes. On the other hand, result of Schwarz et al. [26] is no surface alteration at 100 mJ/pulse, 2 minutes. The different of this is resulted from irradiated area. While it was irradiated on round titanium discs of 10 mm diameter in Schwarz's study, it was irradiated on implant surface area of 2×2 mm2 in our study.
In this study, there was significant surface change between control and test group in SEM image but the difference of roughness value (Ra) on implant surface was not statistically significant. In all test groups except for Nos. 8 and 9, roughness value was slightly increased after laser treatment. The reason is presumed instrument and parameter of roughness measurement. The principle of mechanical contact profilometers is that a pick-up with a stylus is traversed over the surface at a constant velocity. Its disadvantages are that there is no precise information about which regions were actually measured and the surface will be damaged from the load applied on the tip. And it cannot be used for non-destructive evaluations of implants since the tip cannot evaluate threaded parts [39]. Also, the two-dimensional (Ra) or three-dimensional (Sa) parameter of average height deviation is known to be quite stable and insensitive to occasional high peaks or deep valleys and the most commonly used parameter in evaluating implant surface roughness. However, 3D topographic analysis using optical interferometer is superior to 2D analysis because the former (Sa) is more accurate, representative and flexible. Therefore the use of 3D evaluations is recommended for implant surface evaluation [40]. In future study, we will use the instrument and parameter for exact roughness value comparison.
Only the topographic characterization was studied related to the microstructure change in this study. Though surface roughness has been regarded as predominant factor in cell adhesion and osteogenesis during the implant healing phases, no correlation was reported between the profilometry data and bone contact percentage. So additional study is needed that can evaluate the effect of Er:YAG laser on the cell attachment and bacteria removal on the implant surface.
The present study was performed to evaluate the effect of Er:YAG laser irradiation on the change of HA-coated implant surface microstructure according to the laser energy and the application time. In SEM, HA-coated implant surface was not altered by Er:YAG laser irradiation under experimental condition on 100 mJ/pulse, 1 minute, but local areas with surface melting and cracks were founded on 100 mJ/pulse, 1.5 and 2 minutes. In addition, 140 and 180 mJ/pulse group had surface melting and peeling area of HA particles, which condition was more severe depending on the increase of application time. In conclusion, Er:YAG laser on HA-coated implant surface is recommended to be irradiated below 100 mJ/pulse, 1 minute for detoxification of implant surface without surface alteration.





 XML Download
XML Download