

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Generalized aggressive periodontitis (GAgP) is characterized as "generalized interproximal attachment loss affecting at least three permanent teeth other than the first molars and incisors" [1,2].
GAgP affects a minority of patients, but it is highly significant because it is characterized by severe destruction of the supporting apparatus of teeth in a relatively young subjects. Because of its less common occurrence, few studies have evaluated different treatment protocols for this condition. Among those, one study [3] recently applied the principles of full-mouth non-surgical periodontal treatment and found further improvement in clinical parameters when systemically administered antibiotics were added. It has been shown that successful treatment of GAgP is dependent on the reduction of specific pathogenic bacteria.
For example, the adjunctive use of metronidazole plus amoxicillin may control Aggregatibacter actionomycetemcomitans and Porphyromonas gingivalis more efficiently than single antibiotic regimens or mechanical therapy alone [4].
Its etiology is highly correlated to the presence of Aggregatibacter actionmycetencomitans [5-7] and host response defects [8-10] and is possibly related to a genetic inheritance [11-18].
There is no widely accepted treatment protocol for GAgP [19]. Treatment alternatives include scaling and root planing (SRP) alone or in conjunction with systemic antibiotics [20-22] as well as surgical [23] and interdisciplinary approaches [24,25], with adequate outcomes. However, there are only a few reports [19,23,26] of long-term follow-up for these different treatments.
Successful treatment of GAgP is considered to be dependent on early diagnosis, directing therapy towards elimination or suppression of the infecting microorganism and providing an environment conductive to long-term maintenance.
The purpose of this study was to evaluate the improvement of periodontal health of GAgP diagnosed patients treated with non-surgical periodontal therapy accompanying systemic antibiotics administration.
CASE DESCRIPTION
Case 1
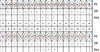
A 28-year-old male patient was referred by a general practitioner to the Institute for Periodontology and School of Dentistry, Kyungpook National University, for treatment of GAgP (Fig. 1). The initial examination revealed deep probing pocket depth (PD) with sulcus bleeding index (SBI). Suppuration was registered at the maxillary right first molar and the mandibular left first molar. Gingival inflammation was observed. The patient was in good general health, had never smoked, and did not take any medications. Familial aggregation of GAgP was denied. PD, tooth mobility (Mob), SBI, and the presence of suppuration were recorded (Fig. 2). A full mouth series of periapical radiographs was obtained (Fig. 3). Deep infrabony defects were evidence of progressing periodontal destruction. After full-mouth scaling, the patient received quadrant root planing four times at 1-weekly intervals over four consecutive sessions. Starting with SRP, systemic antibiotics (amoxicillin/clavulanate 375 mg and metronidazole 250 mg, both three times a day for 7 days) were prescribed. The patient was advised to abstain from mechanical oral hygiene in the treated areas for the first 3 postoperative weeks and to rinse with a 0.2% chlorhexidine solution twice daily. Routine supportive periodontal therapy was performed every 3 months. Whole-mouth clinical measurements were recorded with a manual periodontal probe at 6 month after the initiation of therapy. Measurements demonstrated distinct clinical improvements. PD of the affected sites had decreased to a maximum of 4 mm. Suppuration had been eliminated, and full-mouth SBI was as low as 10%. A negligible increase in recession was observed. Radiographs obtained 1 year after therapy showed fill of the bony defects and sharp contours of the gained hard tissues (Figs. 4, 5, 6).
Case 2
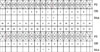
A 12-year-old male patient was referred by a general practitioner to the Institute for Periodontology and School of Dentistry, Kyungpook National University, for treatment of GAgP (Fig. 7). The initial examination revealed deep PD with SBI. Gingival swelling was observed, especially in both anterior areas. The patient was in good general health and did not take any medications. Familial aggregation of GAgP was denied. PD, Mob, SBI and the presence of suppuration were recorded (Fig. 8). A panoramic radiograph was obtained (Fig. 9). Deep infrabony defects were evidence of progressing periodontal destruction. After full-mouth scaling, the patient received quadrant root planing four times at 1-weekly intervals over four consecutive sessions. Starting with SRP, systemic antibiotics (amoxicillin/clavulanate 375 mg and metronidazole 250 mg, both three times a day for 7 days) were prescribed. At supportive periodontal care six month after initial therapy, measurements demonstrated distinct clinical improvements. PD of the affected sites had decreased to a maximum of 7 mm. Full mouth SBI was as low as 5% (Figs. 10 and 11).
DISCUSSION
Several antibiotic regimens have been investigated as adjuncts to the mechanical therapy for GAgP. The combination of SRP with systemic administration of amoxicillin/clavulanate/metronidazole suppressed Aggregatibacter actinomycetemcomitans and other tested pathogens to below detectable levels. The concomitant effect on clinical parameters emphasizes the excellent efficacy of amoxicillin/clavulanate/metronidazole against periodontal infections in terms of microbiologic and clinical outcomes reported previously [20-22, 27].
Because persistently high bacterial counts and the presence of periodontal pathogens at surgery adversely affect clinical attachment level gains [28], meticulous initial therapy and good oral hygiene are considered to be prerequisites for successful periodontal surgery [29].
In case 1, postoperative healing was excellent, facilitated by the systemic administration of antibiotics, which has been reported previously. Six month after therapy, distinct clinical improvements were indicated. PD reduction ranged from 3 to 7 mm. Suppuration had been eliminated, and no gingival inflammation signs were observed. The periapical radiographs obtained 1 year after therapy showed fill of the bony defects and stability of the treatment outcome,. Although all sites demonstrated comparable clinical improvements, varying degrees of radiographic defect fill were observed (Figs. 4-6).
In case 2, substantial and stable clinical periodontal status were shown after conventional periodontal therapy and adjunctive administration of antibiotics. Six month after initial therapy, measurements indicated distinct clinical improvements with redection of PD and no suppuration. And full mouth SBI was decreased.
A high "repair potential" of previously untreated young GAgP patients is empirically assumed and has been a regular subject of discussion. However, the noticeably higher age, which was 28 years, of the patient presented here might limit the clinical application of these findings. Furthermore, after repeated attempts at periodontal therapy with concomitant "mechanical damage" to the root surfaces and subsequent bacterial recolonization and disease progression, the individual healing potential after the initial therapy alone could not be certain for the present patient. To improve the unclear prognosis, the depicted course of treatment included regenerative periodontal surgery, performed shortly after SRP and adjunctive antibiotics therapy.
The combination of initial therapy with adjunctive amoxicillin/clavulanate/metronidazole followed by non-surgical periodontal therapy provided a good clinical, radiographic, and esthetic result in the present patients with severe and progressing GAgP. Beyond the limits of these case reports, the significance of regenerative therapy in the evidence-based treatment of GAgP remains to be evaluated.









 XML Download
XML Download