

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Various treatment modalities have been performed to restore lost periodontal tissue due to periodontitis. First, scaling and root planing are performed to remove local factors such as plaque, calculus and endotoxin. When the inflammatory signs remain at the sites with deep probing pocket depth and alveolar bone defects, periodontal surgery may be necessary.
Periodontal surgeries such as gingivectomy, open flap debridement, modified Widman flap, and osseous surgery are performed to access diseased root surfaces and remove local factors effectively. These procedures result in pocket depth reduction and clinical attachment gain [1-3]. However, these results are usually achieved by the formation of long junctional epithelium without connective tissue attachment or cementum formation [4-6]. This wound healing pattern is considered periodontal repair, not regeneration.
For periodontal regeneration, the gingival epithelium has to be prevented from contacting the root surface during healing. Gottlow et al. [7] showed that a barrier membrane could block the ingrowth of gingival epithelium and connective tissue into periodontal defects.
The guided tissue regeneration (GTR) procedure, in which a barrier membrane is used to exclude soft tissue from the defects, has been shown to partially regenerate lost periodontal tissue with new bone, periodontal ligament, and cementum [8]. Also, the guided bone regeneration (GBR) procedure has been performed for bone regeneration of peri-implant defects [9].
For successful periodontal regeneration by the GTR procedure, the role of a barrier membrane is very important [10]. Therefore, many scientific efforts have focused on the development of effective barrier membranes [11,12]. Non-resorbable membranes have a superior capacity for cell occlusion and space maintenance [13]. However, these membranes have drawbacks, such as frequent membrane exposure and the necessity of a second surgery for membrane removal [14]. Therefore, resorbable membranes are widely used for guided tissue or bone regeneration. Resorbable membranes have been shown to be comparable to non-resorbable membranes with regard to probing depth reduction, clinical attachment gain, and percent of bone fill [15].
Collagen appears to be an ideal choice for resorbable membranes because of excellent biocompatibility and capacity to enhance the wound healing process [16]. In addition, collagen membranes have shown no adverse effect to surrounding tissues during the degradation process [17]. This is another advantage of collagen compared to synthetic materials, such as poly(lactide-co-glycolide) (PLGA), that induce foreign body reactions during degradation [18]. Nevertheless, the degradation of collagen membranes is too fast to maintain the structural integrity necessary for bone/tissue regeneration. To prolong the degradation time of collagen membranes, various cross-linking techniques have been developed. Many studies showed that the higher the degree of cross-linking, the slower the rate of degradation of the collagen membrane [19].
For cross-linking, chemicals such as formaldehyde and glutaraldehyde are added to collagen membranes. These chemicals could adversely influence surrounding tissues. In fact, the glutaraldehyde technique, the most widely used chemical cross-linking technique, was reported to leave a cytotoxic residue during the process [20].
The aim of this study is to evaluate the ability of a porous non-chemical cross-linking porcine-derived collagen nanofibrous membrane to enhance guided bone and associated tissue regeneration in one-wall intrabony defects in beagles.
MATERIALS AND METHODS
Animals
Two adult male beagle dogs with intact dentition and healthy periodontium were used as subjects. Animal selection, management, surgical protocol, and periodontal defect preparation followed routines approved by the Institute of Laboratory Animal Resources at Seoul National University. The animals were provided with a standard laboratory diet and water until the beginning of the study. The animals were provided with a soft diet throughout the study to reduce mechanical interference with healing during food intake. Oral prophylaxis was performed within the 2 weeks prior to the experimental surgeries.
Preparation of membranes
Ten percent collagen solution was made with 5 g collagen and 50 mL hexafluoroisopropanol. The membranes were prepared by electro-spinning the collagen solution and collecting sheets of nano-fibers, followed by cross-linking with heat treatment and the non-chemical method. The cross-linked collagen membrane was prefrozen in a deep freezer for 12 hours and freeze-dried for 24 hours. After freeze-drying, the collagen membrane was dried in the oven at 140℃ for 48 hours. The collagen membrane (Guidoss, NIBEC, Seoul, Korea) was then used in this study.
Surgical procedures
Food was withheld the night before surgery. General anesthesia was induced with 2% xylazine hydrochloride and ketamine hydrochloride. Routine dental infiltration anesthesia with 2% lidocaine with epinephrine (1:100,000) was used at the surgical sites. Under anesthesia, the second and third mandibular premolars and first molars were extracted bilaterally. The extraction sites were allowed to heal for 10 weeks.
After the 10-week healing interval, one-wall intrabony defects were prepared bilaterally on the mesial and distal side of the fourth mandibular premolars. Crestal incisions of 20 mm length were made on the mesial and distal side of the fourth premolars and connected with sulcular incisions made circumferentially. Vertical incisions were made at the end of the crestal incision, followed by periodontal flap reflections. After flap reflection, one-wall intrabony defects sized 4 × 5 mm (mesio-distal width and apico-coronal height, respectively) were created on the mesial and distal sides of the fourth premolars using round and fissure burs with sterile saline irrigation (Fig. 1A). Cementum was removed completely by root planing using Gracey curettes and chisels. Reference notches were made with a #1 round bur on the root surface at the base of the defect, and at the cementoenamel junction (CEJ) for histometric analysis.
Of the two defects of each fourth premolar, one was not covered with a membrane as a control and the other was covered with the collagen membrane (Guidoss, NIBEC, Seoul, Korea) as the experimental group (Fig. 1B).
Membranes were stabilized with fixation screws on each of the defects. After defect management, periosteal-releasing incisions were made to allow for tension-free flap apposition. The flaps were advanced, and sutured slightly coronal to the CEJ (Fig. 1C).
Post-surgical protocol
Post-surgical management of the animals involved intramuscular injection of cefazolin (20 mg/kg) with carprofen (4.4 mg/kg) daily for 3 days, a soft diet, and topical application of a 2% solution of chlorhexidine gluconate three times a week for 10 weeks. The sutures were removed 2 weeks after surgery.
Histologic processing and evaluation
The animals were sacrificed 10 weeks after surgery. All defects were dissected with the surrounding soft and hard tissues. The tissue blocks were fixed in 10% buffered formalin for 3-5 days, decalcified in 5% formic acid for 8-10 weeks, trimmed, dehydrated in an ethanol series, and embedded in the embedding media. Step serial sections were prepared along the mesio-distal plane and parallel with the long axis of the tooth, and stained with hematoxylin-eosin.
Histological and histometric analysis
Analysis was performed using a light microscope (BH-2, Olympus Optical, Osaka, Japan), a microscope digital camera system, and a PC-based image analysis system (Image-Pro Plus, Media Cybernetics, Silver Springs, MD, USA) by one investigator. The following parameters were measured and analyzed (Fig. 2):
Defect height (DH): distance between the apical extension of the root planing and the CEJ.
Junctional epithelium migration (JE): the distance between the apical extension of the junctional epithelium and the CEJ.
New cementum (NC): distance between the apical extension of the root planing and the coronal extension of a continuous layer of new cementum or cementum-like deposit on the planed root.
New bone height (NBh): distance between the apical extension of the root planing and the coronal extension of alveolar bone formation along the planed root.
New bone area (NBa): NBa in the region of interest (ROI)/area of the ROI × 100 (%).
The ROI for NBa was measured by connecting 4 imaginary lines encompassing the defect base and the root surface to establish the region of interest with a shape of a 3 × 3 mm square (Fig. 2). The reason for this establishment was that the proposed standardized defects with the dimensions of 4 mm width × 5 mm height were difficult to create identically during surgery. Therefore, to eliminate any possible errors during evaluation, NBa was measured using an ROI of equal dimensions and position.
Radiographic analysis: micro-computed tomography (CT)
Following fixation, all samples were scanned by a high-resolution micro-CT (SkyScan 1172, SkyScan, Aartselaar, Belgium). Serial tomographic images were acquired transverse to the longitudinal axis of the tooth at 85 kV and 116 µA, collecting 1,200 projections per rotation at 316 ms integration time. Images were produced with a voxel size of 15 × 15 × 15 µm3.
The image data sets were reconstructed to three-dimensional views of the specimens and analyzed using software provided by the manufacturer (CT-Analyser, SkyScan, Aartselaar, Belgium). The percentile new bone volume (NBv) recorded represented the percentage of a volume of the newly formed bone in the region of interest. Various thresholds were applied to differentiate bone from graft particles, soft tissues, and bone marrow.
The region of interest for NBv was established with a cube shape of 4 mm dimensions encompassing the defect base and the root surface. The reason for the establishment of ROI for NBv was the same as the ROI for NBa.
Statistical analysis
The mean and standard deviations of each parameter were calculated for each treatment group using the values obtained from the subjects. Statistical analysis was performed using the software package (SPSS, SPSS Inc., Chicago, IL, USA). A paired Student's t-test was performed to compare data from the in vivo histomorphometric analysis. A P-value < 0.05 was considered statistically significant.
RESULTS
Clinical observations
Wound healing was uneventful at all surgical sites. There were no inflammatory signs following surgical procedures. Other postoperative complications such as wound dehiscence, membrane exposure, infection, and suppuration were not observed during the healing period.
Histologic analysis
In the control group, extensive bone resorption was observed. A crestal bone adjacent to the defect was resorbed to the level of the defect base. With bone resorption, soft tissue was collapsed into the defect. Bone regeneration was minimal. The regenerated bone was limited to the defect notch area. The junctional epithelium apically migrated to the notch on the CEJ. New cementum formation was minimal or not observed (Fig. 3A).
In the experimental group, a crestal bone adjacent to the defect had resorbed to some extent. However, the quantity of newly formed bone was greater than in the control group. Soft tissue collapse was observed into the defect but the extent was minimal compared to the control group. The apical migration of the junctional epithelium terminated within the CEJ notch area (Fig. 3B).
Histometric analysis
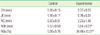
The results of histometric analysis are shown in Table 1. In the apical extension of the junctional epithelium, the experimental group showed a smaller mean value. This result might mean that the membrane prevented the junctional epithelium from undergoing apical migration. However, there was no statistically significant difference between the groups.
For new cementum formation, there was no statistically significant difference between groups. Also, large variations were observed within the same group.
The NBh of the experimental group was greater than the control group. The experimental group showed a significantly greater value of NBh compared with the control group (P = 0.003). Also, for the NBa, the experimental group showed a greater value than the control group, representing a statistically significant difference (P = 0.013).
DISCUSSION
In the present study, one-wall intrabony defects were used to evaluate the effect of a porous non-chemical cross-linking porcine-derived collagen nanofibrous membrane on periodontal tissue regeneration. This defect model is unfavorable for bone regeneration since a positive correlation between the number of bone walls and wound-healing potential exists [21]. In addition, this defect model is a non-contained defect in which is difficult for resorbable membranes to maintain the space. Therefore, it was possible to strictly evaluate the effect of this membrane on periodontal tissue regeneration.
The most remarkable result observed in this study was the effect of this membrane on bone regeneration. For the three parameters used to evaluate bone regeneration, NBh, NBa, and NBv, the experimental group showed superior results compared to the control group, constituting statistically significant differences. These results imply that this collagen membrane enhanced bone regeneration in one-wall intrabony defects. It is noteworthy that these results were attained in an unfavorable defect model for bone regeneration. In previous studies, in non-contained defects like one-wall intrabony defects or supra-alveolar defects, the combined use of a barrier membrane and bone graft showed greater bone formation than only membrane use [13,22,23]. In their systematic review, Sculean et al. [24] concluded that in non-contained defects like supra-alveolar defects, a combination of a barrier membrane and graft material provided superior histologic bone repair results to barrier membranes or graft materials alone. Therefore, more bone regeneration is expected to occur if this collagen membrane is used with a bone graft in this defect model.
For a more accurate evaluation of bone regeneration, three parameters--NBh, NBa, NBv--were used in this study. Through these parameters, new bone formation was analyzed one- (length), two- (area), and three-dimensionally (volume).
NBv was analyzed with micro-CT. Micro-CT has been used extensively to characterize bone tissue and analyze the bone healing process [25,26]. Even though histologic analysis is still considered the gold standard for evaluating bone regeneration in bony defects [27], many previous studies have shown a consistent pattern of bone formation in both micro-CT and histological images [28,29]. In this study, images from the micro-CT were similar to histologic images, similar to the results of previous studies (Fig. 4). In this respect, new bone volume was measured with the micro-CT as a parameter for evaluating bone regeneration.
Unlike bone regeneration, the collagen membrane did not influence periodontal tissue regeneration in the present study. There was no statistically significant difference between the two groups in the apical migration of the junctional epithelium. This finding shows that barrier membranes do not affect the apical extension of the junctional epithelium. Previous studies showed similar results, observing that the apical extension of junctional epithelium was small regardless of the use of a barrier membrane [30,31]. Song et al. [30] reported that there was no significant difference in the junctional epithelium migration between the control and PLGA membrane groups in surgically created one-wall defects in beagles.
New cementum formation was minimal in both groups. Although the experimental group showed a greater mean value compared to the control group, there was no statistically significant difference. Large variations were observed within the same group. On the other hand, in previous studies, cementum regeneration was apparently observed at the GTR site in histologic analysis [32-34]. Sculean et al. [33] reported that new alveolar bone and connective tissue attachment (new cementum with inserted collagen fibers) were regenerated in the intrabony defect after GTR using a resorbable membrane. Therefore, further investigation is necessary to confirm the influence of this membrane on periodontal tissue regeneration.
In summary, the present study confirmed the capacity of the porous non-chemical cross-linking porcine-derived collagen nanofibrous membrane for bone regeneration in a one-wall intrabony defect model. Through various parameters used to evaluate bone regeneration, it was shown that this membrane enhanced bone regeneration at the periodontal defect. On the other hand, the influence of this membrane on periodontal tissue regeneration could not be ascertained within the limitations of this study, and further investigations are necessary.





 XML Download
XML Download