

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The ultimate reason for periodontal treatment is to regenerate the periodontal tissue loss caused by periodontal disease [1-3]. Periodontal regeneration is the healing pattern of new attachment, new bone formation, new cementum and new periodontal ligament. Many approaches are available for regenerating periodontal tissue, including root conditioning, which enhances cell adhesive capacity, bone grafts used for bony defect regeneration, and guided bone regeneration using specific cell migration and bone morphorgenetic protein (BMP) [4] and various other growth factors [5]. BMPs are members of the transforming growth factor-β (TGF-β) superfamily, in which the cytokines induce ectopic bone formation [4,6,7]. Among the BMPs, rh-BMP-2, and -7 [8], which have been synthesized by the DNA technique, are known to have the best osteoconduction. In one study, a composite of gelatin and rhBMP-2 released rhBMP-2 in the proper way and also demonstrated the largest amount of bone formation [9].
BMPs need to be directed to the exact location where bone repair is needed. Recently, there have been studies on the protein transduction domain, which can transmit protein that is difficult to effectively penetrate intracellularly [10]. The phenomenon of the penetration of peptide has shown the possibility of the therapeutic effect of a fast half-life for its fast penetration intracelluarly. Peptides consist of a specific amino acid sequence that can penetrate the cell membrane spontaneously [11,12]. Peptides are short polymers formed from linking α-amino acids in a defined order. The link between one amino acid residue and the next is known as an amide bond or peptide bond. Proteins are polypeptide molecules (or consist of multiple polypeptide subunits). The distinction is that peptides are short and polypeptides or proteins are long.
In this regard, synthetic peptide has been developed with the interest of developing an osteoconductive biomaterial. Significant interest has emerged in the design of cell scaffolds that incorporate peptide sequences that correspond to known signaling domains in extracellular matrix (ECM) proteins [13]. Peptides offer the advantages of increased stability, the ability to incorporate them at much higher concentrations than full proteins, and relatively straightforward and simple syntheses of short sequences [13]. Synthetic peptide was based on BMP-2, which promotes the formation and regeneration of bone and cartilage, and also participates in organogenesis, cell differentiation, cell proliferation, and apoptosis [4].
This synthetic peptide was developed for its various advantages when compared with BMP-2. It is more economical in that the raw material is cheaper than BMP-2. It is very stable in terms of temperature storage. Peptides are known to denaturize at room temperature. However, the sequence is short in the synthetic peptide. It can be stored in a freeze-dried condition for over 2 years. It can also be stored at room temperature in a dry environment, whereas BMP-2 is a cold chain that can only be stored for a short time, for example, 6 months at 4℃.
On this basis, the purpose of this study was to evaluate the effects of bone regeneration of synthetic peptide in surgically created rat calvarial defects.
MATERIALS AND METHODS
Animals
Forty male Sprague-Dawley rats (body weight, 200 to 300 g) were used in this study. Animal selection and management, surgical protocol, and preparation followed the routines approved by the Institutional Animal Care and Use Committee of Yonsei Medical Center in Seoul, Korea.
Experimental group design
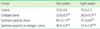
The animals were divided into four groups of 10 animals each and allowed to heal for 2 weeks (5 rats) or 8 weeks (5 rats) as shown in Table 1. Each animal was categorized as either one of four groups: a sham-surgery control group in which no material was applied to the defect, collagen carrier alone group, synthetic peptide alone group, or both synthetic peptide in collagen carrier group.
Designing of the synthetic peptide
The significant amino acid sequences in growth factors and ECM, both of which are involved in bone formation, the early attachment, proliferation, and differentiation of the osteocyte, were analyzed among the whole amino acid sequence of the following proteins; BMP-2, fibronectin, and vitronectin. In the case of BMP-2, bone forming cells, i.e., osteoblasts, have a specific binding site and in terms of the ECM, considering that the sequence is involved in cell attachment, the synthetic peptide was recombined based on the sequence. The osteoblasts can recognize the sequence of synthetic peptide as an active domain of the protein, so synthetic peptide was recombined to induce attachment, proliferation, and differentiation. N- and C-terminals were stabilized through amidation, and acetylation. Of all the amino acid sequences of BMP-2, fibronectin and vitronectin, the amino acid sequence that plays the core role in the proliferation and differentiation of osteoblasts was selected and analyzed. A part of these sequences was modified by peptide synthesizer and the synthetic peptide was formed. The final product after synthesis was purified to a level over 95% using high pressure liquid chromatography and the mass was analyzed through nuclear magnetic resonance. The synthesis and purification of synthetic peptide was consulted with Shimadzu Co., Ltd. A Prominence HPLC (Shimadazu Co., Kyoto, Japan) was used to determine the flow rate, which was 1.0 mL/min and the detection was performed at 220 nm and was purified at 98.6%. The concentration of the synthetic peptide was loaded with 10 µL (mass: 2,288) (application number: 10-2008-54730 [08.6.11], registration number: 10-879704 [09.1.13]).
Surgical protocol
The animals were anaesthetized by an intramuscular injection (5 mg/kg body weight.) consisting of ketamine hydrochloride (Ketalar™, Yuhan Co., Seoul, Korea). Routine infiltration anaesthesia with 2% lidocaine and 1:100,000 epinephrine (Kwangmyung Pharm., Seoul, Korea) was used at the surgical site. An incision was made in the sagittal plane across the cranium and a full thickness flap was reflected, exposing the calvarial bone. A standardized, circular, transosseous defect, 8 mm in diameter, was created on the cranium with the use of a saline-cooled trephine drill (Biomet 3i, Palm Beach Gardens, USA). After removal of the trephined calvarial disk, absorbable collagen membrane 1 cm × 1 cm (Collatape™, Integra Life-Sciences Co., Plainsboro, USA), the carrier and synthetic peptide were applied to the defects. The animals were divided into four groups of 10 animals each and allowed to heal for 2 (5 rats) and 8 (5 rats) weeks. Each animal received one of three experimental conditions: synthetic peptide only, collagen only, or both synthetic peptide and collagen. The periosteum and skin were then closed and sutured with 4-0 Monosyn (Aesculap Inc., Center Valley, USA).
Evaluation methods
Specimen preparation
The animals were sacrificed by CO2 asphyxiation at 2 or 8 weeks post-surgery. Block sections including the experimental sites were removed. Samples were fixed in 10% neutral buffered formalin solution for 10 days. Samples were decalcified in 5% formic acid for 14 days and embedded in paraffin. Serial sections, 5 µm thick, were prepared at intervals of 80 µm, stained with Hematoxylin/Eosin and examined using a light microscope. The most central sections from each block were selected to compare histologic findings among the groups.
Histomorphometric analysis
Computer-assisted histometric measurements were obtained using an automated image analysis system (Image-Pro Plus®, Media Cybernetics, Silver Spring, USA) coupled with a video camera on a light microscope (Olympus BX50™, Olympus Optical Co., Tokyo, Japan). Sections were examined at 20×magnification. A digitizer was used to trace the defect outline versus new bone formation, and a percentage of bone fill was determined. The following histomorphometric parameters were measured from each sample (Fig. 1):
Defect closure (%): the distance (at each side of the defect) between the defect margin and the in-growing bone margin in millimeters × 100.
New bone area (mm2): all tissues within the boundaries of newly formed bone, i.e., mineralized bone and fatty marrow and fibrovascular tissue/marrow and residual biomaterial.
Bone density (%): the newly formed bone within the new bone area in millimeters × 100.
Statistical analysis
Histomorphometric recordings from the samples were used to calculate means and standard deviations (mean ± SD). To analyze the effect of both time and condition and to detect the interaction effect between time and condition, two-way analysis of variance was used (P < 0.05). ANOVA and a Post hoc test were used to analyze the differences among the groups at each point in time (P < 0.05). For the comparison between 2 and 8 weeks in the same group, statistical significance was determined by a paired t-test (P < 0.05).
RESULTS
Clinical observations
Wound healing was generally uneventful and appeared similar for the experimental groups. Material exposure or other complications of the surgical sites were not observed.
Histologic observations
Sham-surgery control group
Two weeks
At 2 weeks post-surgery, the defect was filled with thin, loose connective tissue. The control group showed minimal new bone formation originating from the defect margins (Fig. 2).
Eight weeks
At 8 weeks post-surgery, there was a relatively consistent density of connective tissue around minimal new bone formation. However, loose connective tissue could still be observed. The bone forming cells, osteoblasts, were observed at the bottom of the new bone formation (Fig. 3).
Collagen alone group
Two weeks
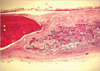
The defects were filled with loose or dense, fibrous connective tissue and limited new bone formation was observed at the defect margin at 2 weeks. Collagen remained in the subepithelium, there was no resorption, and it maintained the external form and was surrounded by connective tissue (Fig. 4).
Eight weeks
The resorption of the collagen progressed greatly. There was almost no infiltration of inflammatory cells. There was an increase in bone volume and there was no invagination of the peripheral tissue (Fig. 5).
Synthetic peptide alone group
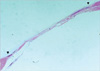
Two weeks
There was almost no resorption and there was slightly new bone formation and a slight increase in volume as well. There was not much defect closure yet at 2 weeks. The margin was differentiated from the peripheral tissue (Fig. 6).
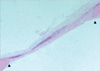
Eight weeks
There was a great amount of resorption. The new bone formation increased compared to the 2 weeks' group. There was resorption; however, the exterior was roughly maintained. There was a greater closure compared to the 2-week group. Osteoblast-like cells and a very few giant multinucleated cells could be detected in the periphery of the margin whereas the center showed almost no new bone formation (Fig. 7).
Histomorphometric analysis
The results of the histomorphometric analysis are shown in Tables 2, 3, 4. There was minimal new bone formation in the control group. At all time points, defect closure and new bone in all experimental groups were significantly different from that in the control group (P < 0.05).
At 8 weeks, the collagen group showed a significantly greater defect closure and new bone area than the synthetic peptide group (P < 0.01). There were statistically significant differences between the results obtained at 2 and 8 weeks in the collagen group (P < 0.05). There was no significant bone growth in the synthetic peptide (no carrier), whereas there was an increase at 2 and 8 weeks in the synthetic peptide and collagen group.
DISCUSSION
The purpose of this study was to evaluate the bone regenerative effects of the synthetic peptide in a critical-size rat calvarial defect model. Eight-millimeter-diameter standardized, circular, transosseus defects created on the cranium of rats were implanted with synthetic peptide, collagen, or both synthetic peptide and collagen. The healing of each group was evaluated histologically and histomorphometrically after 2- and 8-week healing intervals.
The critical-size rat calvarial defect used in this study was a very convenient model for evaluating bone regenerative effects of biomaterials. This model is relatively accessible, simple, and reproducible because spontaneous healing does not occur in the control specimen [14]. It has been shown effective to evaluate the potential for bone formation [15-18]. In addition, after bone augmentation, this model has some compressive force, which is similar to intraoral conditions. It has many similarities to the maxillofacial region, as anatomically the calvaria consists of two cortical plates with a region of intervening cancellous bone similar to the mandible, and physiologically, the cortical bone in the calvaria resembles an atrophic mandible. Other advantages are that the observation can be focused on the healing process of the bone, since there are no major nerves or blood vessels around the rat calvaria and that the parameters can be simply and accurately measured in each specimen.
The materials that were used were the synthetic peptide and collagen. The synthetic peptide has been developed with the interest of developing an osteoconductive biomaterial. Based on many studies of effective results of BMP-2, the synthetic peptide consists of 21 amino acid sequences, with an alteration of just one amino acid sequence from the entire BMP-2 sequence [19].
The amount of the synthetic peptide used was 10 µL loading (mass, 2,288). This was ten times that of the BMP-2 concentration. The amount was set based on the cell test and 100 times that of the actual concentration is thought to be the best concentration. Gel type was used to reduce the volume and the ease of use.
In the present study, collagen stabilized the gel type of the synthetic peptide, which has a disperse effect. When the synthetic peptide was used with collagen, the effect was enhanced and the results were significant when compared with the control groups or when used with a single biomaterial.
In histometric analysis, the defect closure, new bone area, and bone density were compared. The specimen was obtained from the middle coronal section. The measurement of length of the new bone formation is to compare the amount of cell migration. The further the cells migrate, the higher the possibility of bone union. As the length growth of the cells increases, in considering the thickness, more bone formation could be predicted. Therefore, this could be said to be a good marker for a membrane's bone regenerative capacity.
Irrespective of the types of bone graft material used, all defect sites exhibited bone formation in a similar pattern and there was more new bone formation at 8 weeks than at baseline. At 2 weeks, a parallel pattern within was observed and newly formed bone without any significant adverse reaction was seen. Newly formed bone with osteocytes was evident mainly at the periphery of the defects, and osteoblast-like cells exhibiting a dense arrangement adjacent to the newly formed bone suggest continued bone apposition at the initial healing stage. However, less bone formative activity was found at the central aspects of the defects. Multinucleated giant cells were observed in the periphery of the synthetic peptide material. There was no evidence of fatty marrow or cartilage formation.
At 8 weeks, the quantity of the new bone was greater than that observed at 2 weeks and the specimen showed a more advanced stage of remodeling and consolidation. The newly formed bone consisted of woven bone and lamellar bone, and showed cement lines separated earlier from more recently deposited bone and concentric rings of the Haversian system. However, collagen remnants and dense arrangement of osteoblast-like cells were detected at 8 weeks. There was no evidence of fatty marrow or cartilage formation.
In tissue engineering technique, the key concept is that an isolated cultured cell on a scaffold is transplanted into the target tissue for its regeneration [20]. Many studies have reported that BMP-2 is effective in bone formation [21] when combined with a carrier, such as collagen or decalcified bone [12-24]. In the present study, collagen was mostly absorbed, forming new bone. This was more prominent at 8 weeks. No significant differences were seen between the time intervals. 2 and 4 weeks could have been a better comparison. In addition, the liquid type of synthetic peptide could have been lost around the rim for its disparity. This could be changed to granules or a powder type or could be reinforced with a carrier. When used with the synthetic peptide and collagen, the new bone formation was enhanced. The concentration could be altered through further studies. The experimental group design and different time interval may have yielded better results. The synthetic peptide was developed to be effective in a minimal gap in osseous defects during implantation. However, in the present study, a whole defect model was used. When embedding this material in implants, it could be possible to enhance bone formation with a scaffold such as collagen membrane, which would also increase the stability of the material [25].
Although the synthetic peptides seem to be effective in periodontal tissue regeneration, they still need further research on its suitable sequences and optimal concentration for this goal.









 XML Download
XML Download