

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Surgical management of acetabular fractures is complex and continuously evolving. The use of periacetabular screws to treat acetabular fractures remains common and is technically demanding due to the narrow osseous corridors in the helical-shaped innominate bone and challenges in visualizing the hip joint surface1). Perforations associated with the treatment of acetabular fractures with periacetabular screws are reported to occur between 0.9% and 7.0%2), and are a potentially serious complication that may cause severe and rapid destruction of the articular cartilage, leading to osteoarthritis of the hip joint. When intraarticular screw perforation is identified on a postoperative computed tomography (CT) scan, removal of the screw is required.
Removal of a periacetabular screw causing a perforation typically requires a sizable dissection, exposing the patient to considerable risk of morbidity and a significant recovery time. For this reason, the identification of a less invasive surgical procedure capable of achieving results similar to conventional treatment is highly desirable. Recent advances in hip arthroscopy make it possible to gain less invasive access to the hip joint compared with standard open surgical techniques. Here, we describe the safe and effective arthroscopic removal of a screw perforating the hip joint following surgical treatment of a posterior acetabular wall fracture.
CASE REPORT
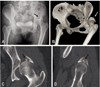
The patient was informed that this case would be submitted for publication. A 50-year-old woman was involved in a car crash and sustained a left posterior acetabular wall fracture with posterior hip dislocation (Fig. 1). Although closed reduction was performed in the emergency room, the left hip joint seemed unstable. Open reduction and internal fixation using a reconstruction plate and screws were performed 6 days after admission. The Kocher-Langenbeck approach was used to access the hip joint. The fracture had completely displaced multiple fragments, including osteochondral free fragments. Using the femoral head as a template, open reduction of small free fragments was performed to restore articular congruency. In the metaphyseal defect underneath the small osteochondral fragment, cancellous autografting was performed to fill the defect. Thereafter, the osteochondral fragments were fixed with a full-threaded titanium cortical screw measuring (2.0 mm diameter). This screw was embedded underneath the posterior wall fragment to fix the osteochondral fragment. After two large fragments were fixed using full threaded cortical screws (2.0 and 3.5 mm in diameter), buttressing plating with a 3.5 mm undercontoured reconstruction plate was performed (Fig. 2A, B). We used intraoperative fluoroscopy to monitor the screw position and ensure that there was no definite evidence of intra-articular screw penetration.
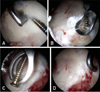
Following surgery, the patient complained of left hip pain during range of motion exercises, and her general condition required a CT scan 1 month after surgery. The results of this CT scan revealed intraarticular perforation of the cortical screw used to fix a small osteochondral fragment (Fig. 2C, D) and removal of the intraarticular perforated screw using hip arthroscopy was undertaken. All procedures were performed under general anesthesia, with the patient in the supine position with the extremity in traction on a fracture table. Traction was applied to the left hip joint of the patient until about 8 to 10 mm of joint space separation was obtained. To access the central compartment, an anterolateral portal for viewing and an anterior portal for working were made using fluoroscopy. The posterolateral portal was used only for outflow. The intraarticularly penetrating screw was oriented in the 2 o'clock to 10 o'clock direction (Fig. 3A). Articular cartilage surrounding the screw was removed using an extra small arthroscopic gauge and ring curette for hip arthroscopy to expose the whole penetrated screw. Special care was taken not to remove excess cartilage. The screw head, which was placed underneath the osteochondral fragment, was exposed after removing the subchondral bone using an extra small arthroscopic ring curette for hip arthroscopy (Fig. 3B). After checking the motion of the screw, we removed the screw using an arthroscopic grasper for hip arthroscopy (Fig. 3C, D). Although some damage to the articular cartilage of the femoral head was observed, we were unable to distinguish the cause of damage (i.e., penetrated screw or initial injury). The quality of acetabular reduction seemed to be acceptable and no evidence of labral injury was observed.
One year after arthroscopic removal of the screw, the follow-up CT scan revealed a small defect in the posterosuperior portion of the acetabulum. However, no radiological signs of osteoarthritic changes were observed (Fig. 4). At this follow up, the patient had full range of motion, no hip pain and was able to ambulate with a normal gait without support.
DISCUSSION
Hip arthroscopy has evolved dramatically since the 1990s3), including advances in surgical techniques, instrumentation, better defined applications, and positive surgical outcomes have been continuously reported4567). Based on these technical advancements of hip arthroscopy, we believed that it may be applied to the removal of a screw perforating into the joint space-one potentially serious complications of open reduction of an acetabular fracture. In addition, we hypothesize that it might prevent the morbidity of arthrotomy and make postoperative rehabilitation much easier with better outcomes8).
Hip arthroscopy is a minimally invasive technique that reduces the morbidity of hip arthrotomy and damage to important muscles, nerves, and vessels, thereby preserving hip function. However, during this arthroscopic procedure and postoperative follow-up period, concerns remain. The first area of concern relates to the loss of articular cartilage. To remove the perforated screw from the joint space, we had to remove some part of the articular cartilage that covered the screw. Although special care was taken to minimize loss of articular cartilage, this might be associated with the progression of traumatic osteoarthritis. Another concern was the potential for a focal joint depression caused by the removal of the perforated screw. This would have offered another chance for traumatic osteoarthritis, if the joint space depression caused instability of the joint or became one of the sources that lead to continuous damage of articular cartilage. Nevertheless, there were two reasons to select arthroscopic technique vs. an open technique in the case. First, the screw was embedded to fix the osteochondral fragment, suggesting that screw removal using open technique would be far more difficult. Second, we believed that arthroscopic technique was technically faster, easier, and less invasive than open technique.
The 1-year follow-up CT scan showed good congruency of the hip joint without considerable loss of articular cartilage or serious joint depression. We believe that these are positive radiological outcomes mainly associated with firm fixation using the lag screw and plate augmentation of the posterior wall, which prevented instability of the hip joint. Additionally, the extent of cartilage damage was not as significant as anticipated, the location of articular defect was more posterior to the weight-bearing portion of the hip joint, and a period of 30 days from operation to screw removal might have a positive effect on the prevention of joint depression.
There are limitations to this case report. First, the size of the screw we removed was only 2.0 mm in diameter and arthroscopic removal of a larger screw will likely be more difficult. Second, we could not consider any surgical treatment for the articular defect after screw removal. Additional techniques, such as bone grafting, autologous osteochondral transplantation, or autologous cartilage implantation, may be need if the defect is more considerable910). Third, a 1-year follow-up may be too short to judge the progress of postoperative arthritis. Further follow-up should be needed. Nevertheless, to the best of our knowledge, this is the first report using the hip arthroscopic technique to treat an intraarticular screw perforation after acetabular fracture.
In conclusion, we describe successful arthroscopic management of an intraarticular screw perforation of the hip after surgical treatment of an acetabular posterior wall fracture. Thus, this technique may offer another surgical option to solve the complication of intraarticular screw perforation if the surgical technique is continuously developed.


 XML Download
XML Download