

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Femoroacetabular impingement (FAI)-a condition characterized by morphologic abnormalities of the hip joint at the junction between the femoral head and neck and the acetabulum during hip movement-was first described by Ganz et al.1) in 1991. Based on abnormal hip morphology, FAI is classified into three types: i) cam-type impingement (characterized by insufficient offset resulting from prominence at the flattened or slightly convex femoral head-neck junction), ii) pincer-type impingement (when the acetabular edge excessively covers the femoral head), and iii) a combination of the two. In cam impingement, bony prominence on the femoral neck impinges on the anterolateral rim of the acetabulum, leading to articular cartilage breakdown and acetabular labral tears. Pincer impingement is caused by abnormal contact between the femoral neck and the anterolateral acetabulum, which results in labrum and articular cartilage damage. FAI has been identified as an early cause of hip osteoarthritis and a contributor to reduced range of motion and decreased hip function234). This condition is known to be particularly common among professional athletes56) with excessive hip movement and individuals involved in yoga or pilates requiring excessive flexion and internal rotation of the hip.
FAI is recognized as a leading cause of hip pain in younger adults and may lead to degenerative arthritis of the hip27), with an estimated prevalence between 10% and 15%8). In recent years, FAI is considered one of the major causes for pain and degenerative arthritis in hip joint among young people involved in aggressive sporting activities. For this reason, early recognition and appropriate management of FAI can prevent progression to hip osteoarthritis9).
One of the indicators used in evaluating deformity at the femoral head-neck junction is alpha angle measurement10), an alpha angle of greater than 55°is considered an indication of the presence of cam-type FAI. Recent studies (in predominantly western populations) have measured the alpha angle by dividing the femoral region into several sections using a clock-face system to three-dimensionally identify morphological abnormalities of the femoral neck and acetabulum using computed tomography (CT) or magnetic resonance imaging (MRI) of the proximal femur111213). Although earlier studies of Korean populations have investigated FAI prevalence using radiography, limitations have been observed in three-dimensionally analyzing morphologic abnormality in the femoral head-neck junction1415). For this reason, there are insufficient data to rule out healthy Korean adults in primary care clinics based on the findings of plain radiography alone due to the paucity of tomographic image data available on FAI in the Korean population.
Therefore, we aimed to investigate: 1) the frequency of radiographic findings of cam FAI in asymptomatic adults, 2) the distribution of cam impingement on three-dimensional (3D) radiographic images of the femoral head-neck junction, and 3) gender differences present in the radiological parameters associated with cam deformity using CT scans of hips among the Korean population.
Go to : 
MATERIALS AND METHODS
There was no institutional review board (IRB) approval due to its retrospective study design.
CT images of the hips of trauma patients who visited Ajou University Hospital from January 2011 to December 2015 were evaluated. This retrospective study involved adults younger than 55 years of age, and, by using their electronic medical record (EMR) data, excluded those suspected of osteoarthritis of the hip and osteonecrosis of the femoral head in the contralateral hip, or associated with pain due to Legg-Calvé-Perthes disease and developmental dislocation of the hip. Of the 100 total patients (100 hips), 51 and 49 were male and female, respectively, with a mean age of 38.5 years (range, 20–54 years). Mean height was 166.4 cm (range, 147–186 cm), mean body weight was 62.5 kg (range, 38–95 kg), and mean body mass index was 22.4 (range, 15.2–30 kg/m2) (Table 1).

Table 1
Baseline Characteristics
![]()
CT scans (Somatom Definition Edge; Siemens, Munich, Germany) were generated with patients in a supine position at a 3-mm slice thickness. The alpha angle was assessed by measuring the angle along the long axis of the femoral neck at clock-face positions of 30°intervals on each sectional image of 3D reconstructions of the proximal femur using Picture Archiving Communications System (PACS) and INFINITT Xelis software (Xelis software, version 1.0.2.2; Infinitt, Seoul, Korea)16). Measurements of alpha angles were made in different regions, each representing a one-hour interval by the clock position from a line drawn between the center of the femoral neck at its narrowest point and the center of the femoral head (at the 12 o'clock [superior], 3 o'clock [anterior] and 9 o'clock [posterior] position). The 12 o'clock position was defined as the superior aspect of the proximal femur in a standing position. The most superior aspect was 12 o'clock, the anterior aspect was 3 o'clock and the posterior aspect was 9 o'clock (Fig. 1). The alpha angle is described as the angle between a line drawn between the center of the femoral neck at its narrowest point, bisecting the circle, and a line connecting the center of the femoral head to a point where the femoral head extrudes a circle drawn around the femoral head. An alpha angle of more than 55°was considered a significant indicator of cam-type impingement. In the current study, an alpha angle of greater than 55°was considered as loss of sphericity of the femoral head and cam FAI (Fig. 2). Statistical analysis was performed using IBM SPSS Statistics ver. 22.0 (IBM Co., Armonk, NY, USA). Data were expressed as means±standard deviations (range). Gender differences were examined using the independent samples t-test and P-values were considered significant at P<0.05. Prevalence difference in each section was analyzed with ANOVA and P-values were considered significant at P<0.05.
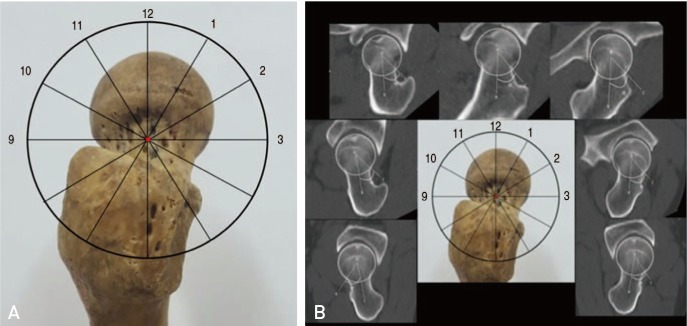 | Fig. 1(A) The 12 o'clock position was defined as the superior aspect of the proximal femur in a standing position. (B) The alpha angle was assessed from the line drawn between the center of the femoral neck at its narrowest point and the center of the femoral head at clock-face positions at 30°intervals using three-dimensional reconstruction of computed tomography imaging of the femur.
|
 | Fig. 2Point A is the center of the femoral head and the line drawn from A to B is the long axis line connecting the centers between the femur head and neck. The line drawn from A to C is the line extending from the center of the femoral head to the point the femoral head extrudes a circle drawn around the femoral head. The angle formed between these two lines is defined as alpha. The alpha angle is described as the angle formed by the femoral neck axial line and the line from the center of the femoral head to a point where the femoral head extends outside the circle around the femoral head.
|
Go to :
RESULTS
The mean age of male (n=51) and female (n=49) patients was 37.5±9.0 years (range, 19–54 years) and 39.5±9.6 years (range, 20–54 years), respectively. The prevalence of radiological findings of cam FAI in asymptomatic adults was 31%. When alpha angles were measured on varying clock-face positions in CT reconstruction, the prevalence of abnormal morphology was 31.0% (31 cases); 37.3% (19 cases) among males and 24.5% (12 cases) among females (Table 2).

Mean alpha angles from 3 to 10 o'clock positions were greater in men than in women, but no statistically significant difference was found in rest positions. As shown in Fig. 3, mean alpha angles were 43.5°, range 34.7–56.1°(3 o'clock); 51.24°, range 39.5–58.8°(2 o'clock); 52.45°, range 43.3–65.5° (1 o'clock); 44.09°, range 36.8–49.8°(12 o'clock); 40.71°, range 33.5–45.8°(11 o'clock); and 39.21°, range 34.1–44.6° (10 o'clock) (Table 3).
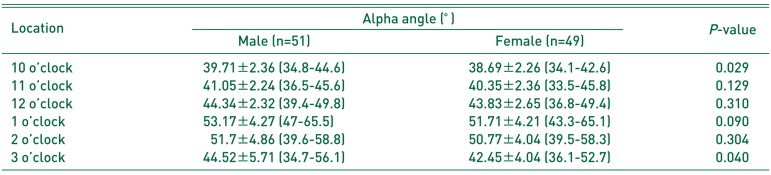
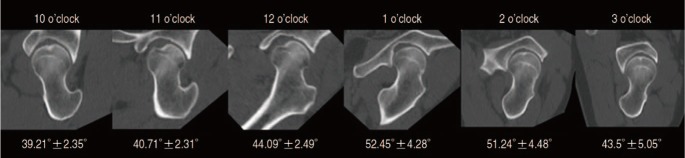
Table 3
Mean Alpha Angle at 10 O'clock to 3 O'clock (by Gender)
![]()
The mean alpha angle was greatest at 1 o'clock and larger than alpha angles at other positions, excluding the angle at 2 o'clock, and these differences were statistically significant. The mean alpha angle at 2 o'clock was the second highest and statistically significantly greater than all other positions excluding 1 o'clock. Even though alpha angles were measured in asymptomatic adults, 31 cases had an alpha angle greater than 55°at 1, 2 and 3 o'clock positions in 18, 19 and 4 cases, respectively. Alpha angles greater than 55°occurred at 1, 2 and 3 o'clock positions (11 cases at 1 o'clock, 13 at 2 o'clock, and 4 at 3 o'clock) in men and at 1 and 2 o'clock positions (7 cases at 1 o'clock and 6 at 2 o'clock) in women (Table 4).

Table 4
Distribution of Alpha Angle >55°Relative to Radial Image Locationz
![]()
The prevalence by age was 8% (20s), 11% (30s), 8% (40s) and 4% (50s) and these differences were no statistically significant (P>0.05).
Go to :
DISCUSSION
Plain radiography is initially performed to screen patients suspected of FAI to determine bony morphologic abnormalities in the femoral head and neck. FAI can be diagnosed when a physical examination reveals morphologic abnormalities that may cause pain, loss of sphericity of the femoral head due to bony prominence on the femoral neck and impingement resulted from excessive coverage of the femoral head by the acetabulum. However, FAI requires comprehensive diagnosis and interpretation of clinical signs and evaluation, since abnormal radiographic findings of the hip can also be found in asymptomatic patients.
Plain radiography is commonly used to diagnose FAI, while MRI and MR arthrography (MRA)2) are useful in identifying labral tears or other hip joint lesions. CT scans can more precisely examine bony morphologic abnormalities by creating 3D images of the bone.
The alpha angle is a radiological parameter used to determine the likelihood of cam deformity that presents abnormal morphology of the femoral head. Nötzli et al.10) measured alpha angles in the anterior region (3 o'clock) of the femoral head in 39 patients with symptomatic and asymptomatic FAI patients using MRI. The mean alpha angle was 42°(range, 33–48°) in the asymptomatic group and 74°(range, 55–95°) in the symptomatic group, and an alpha angle greater than 55°was considered abnormal. However, Neumann et al.17) documented that the average alpha angle for 45 patients who underwent surgery for cam FAI management was 66°preoperatively and 43° postoperatively. They recommended more strict clinical criteria than Nötzli et al.10) by sugesting that patients with an alpha angle of less than 43°at the normal acetabulum may be asymptomatic. Based on this previous method for measurement, we found out that the average alpha angle was 43.5°(range, 34–56°) at the anterior femoral head, comparable to the results of previous studies; however, some asymptomatic patients had an alpha angle greater than 55°. For this reason, caution seems prudent when evaluating the potential for developing FAI in which symptoms may be manifested depending on hip range of motion.
Most prior studies on FAI have involved symptomatic patients1819). Nevertheless, recent data from CT scans have demonstrated a high prevalence of FAI among asymptomatic individuals among Asian populations. Kim et al.15) reported that patients with an alpha angle greater than 55°accounted for 18% and those with a center edge angle greater than 40°accounted for 27% of 473 asymptomatic cases on CT images of the hip. The study was performed with CT scanning by measuring the alpha angle of a single location. On the contrary, the current study identified a difference in prevalence by measuring alpha angles taken at different locations not measured by Kim et al15).
According to another previous study14) conducted with 400 hips, the prevalence of an alpha angle greater than 55°was 5% on Sugioka view. Of these, the prevalence was 12% among males and 1.6% among females. The prevalence of an alpha angle greater than 55°was 8% on 45°Dunn view; 16% among males and 3.5% among females. In the present study, we measured alpha angles on CT images of asymptomatic patients using a clock-face system. This study seems meaningful in that it first carried out measurement on CT images using a clock-face scheme in asymptomatic Korean population, and measured data will be useful in future clinical research.
In previous studies comparing alpha angles measured in different orientations, by rotating a radial plane around the femoral head-neck axis, to identify morphologic abnormalities of the femoral head-neck junction three-dimentionally, the majority of injury occurred in the anterior and superior regions of the hip102021) during hip flexion movement.
Rakhra et al.12) accessed alpha angles at 4 different positions of MRI scans by rotating the planes around the femoral head-neck axis, and the distribution of the maximum alpha angles was most commonly observed at 1 and 2 o'clock positions from the anterior to the superior regions. The maximum alpha angles were 64.7°(range, 44.2–97.5°) at 1 o'clock and 65.9°(range, 44.2–99.3°) at 2 o'clock, and the largest alpha angles were most commonly distributed between the anterior and superior regions. In an investigation on 400 hips of 200 healthy individuals without hip conditions, pain or a history of hip surgery, Hack et al.22) documented that the mean alpha angle was 40.78°(range, 27–69.9°) in the anterior region (3 o'clock) and 50.15°(range, 32.6–76.3°) in the anterior-superior region (1:30 o'clock). Sutter et al.23) reported that the largest alpha angle was 53.3°in the anterior-superior region when alpha angle measurements were made at 5 different positions among normal adults without hip pain. The authors compared alpha angles measured in six different planes rotated around the femoral head-neck axis, and as a result, the highest alpha angle values were located in the anterior-superior region (1 o'clock, 52.45°and 2 o'clock, 51.24°), aligning with previous research. Our study is thought to be meaningful in that it first reviewed alpha angles in six different planes rotated around the femoral head-neck axis in asymptomatic Korean adults.
Siebenrock et al.624) and Agricola et al.25) suggested that cam-type impingement is more prevalent among men than women because of gender-related anatomical differences of the femur and excessive physical activity in male adults. In our study, the prevalence of cam deformity was 37.2% in men and 24.4% in women, aligning with the results of previous studies.
In a study of healthy Asian and European adults with no hip pain by Van Houcke et al.11), the mean alpha angle of the anterior-superior portion (1:30 o'clock) was 52°in Asian men and 49°in Asian women (P<0.001); and 56°in both European men and women (P=0.01). Of those, the prevalence of cam deformity (alpha angle >55°) was 22% in Asian men and 15% in Asian women; and 35% in European men and 32% in European women. The difference in alpha angle between Asian males and females was statistically significant, while no statistically significant difference was observed between European males and females. In the current study, the mean alpha angle of the anterior-superior portion (1 and 2 o'clock) was greater in men than in women, but this difference was not statistically significant. The percentage of adults who could be diagnosed as cam deformity at 1 o'clock was 21.6% among men and 14.6% among women and at 2 o'clock was 25.5% among men and 12.2% among women. These findings are comparable to the results of earlier studies on the prevalence of cam FAI in Asian adults. A lower prevalence than that of cam FAI in European adults is thought to have resulted from racial difference.
Nepple et al.26) compared CT images by dividing from the anterior to the superior portions of the femur at 30° intervals using a clock-face system with plain radiographs (anteroposterior pelvis, 45°Dunn and and frog-leg lateral views). As a result, they reported that the angles of the superior, anterosuperior and anterior regions were identical to those measured in AP pelvis 45°Dunn and and frog-leg lateral views, and cam deformities can be diagnosed using these three plain radiographic techniques instead of CT with increased radiation exposure. In addition, they suggested that the sensitivity was even higher that CT because deformities undetected between 1 and 2 o'clock (1:30 o'clock) can be detected on Dunn view radiographs. Although we were unable to compare regions divided into the clock-face positions with plain radiographs, we evaluated morphologic abnormalities of the femur three-dimensionally using 3D-CT reconstructed images and reported normal ranges in each location.
In our study, the prevalences of cam deformity at 1, 2 and 3 o'clock positions are 18.0%, 19.0% and 4.0%, respectively. Moreover, 31 hips (31.0%) had a cam deformity in at least one location, and 8 hips (8.0%) had two or more cam deformities. The difference in prevalence by location seems to imply that cam impingement observed in two or more positions can be detected by screening for cam deformity in one area on plain radiographs, but cam deformity in other areas can be overlooked. Evaluating the prevalence of cam-type FAI using CT scans is thought to be meaningful and a strength of this study.
This retrospective study was limited in certain aspects. First, the sample size (n=100 hips) was relatively small. Second, since the authors reviewed the subjects based on EMR, the actual physical examination and follow-up were not carried out to confirm asymptomatic hip. Third, the presence of correlation and secondary deformity were not evaluated through radiographic measurements of pincer-type impingement, and the alpha angle was measured by a single person.
Go to :
CONCLUSION
The prevalence of imaging features of cam-type FAI on CT was 31% in asymptomatic Korean adults. Cam deformity was commonly observed in the anterosuperior region of the femoral head-neck junction. There was a gender difference in prevalence, but the differences were not statistically significant.
Go to :
 XML Download
XML Download