

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Several adult femoral neck stress fracture cases have been reported. It is well-known that most of the cases occur in athlete123) and military recruit populations45). Such kind of fracture that occured in other adult group of patients (non-athlete/military) is very uncommon. Unfortunately, sometimes plain radiograph could not show any clear finding4). Hence they were often to be missed and caused significant displacement which required surgery6).
We report a case of bilateral femoral neck stress fracture in a male shipman laborer who complaint only unilaterally at the presentation.
CASE REPORT
A 37 year-old male presented 3 weeks history of unilateral left groin pain and anterior thigh pain especially after weight-bearing activities. The pain was dull and non-radiating. He denied any history of symptoms on the right hip. There was no history of trauma, alcohol abuse, steroid use metabolic disorder, and any relevant diseases.
His job involves lifting heavy object at a cargo ship. Almost everyday, he lift several object with weight approximately 30-50 kg in 8-10 hours of working time a day. His body height was 175 cm with body weight 73 kg, and his body mass index was 23.8 kg/m2. At presentation, physical examination revealed no deformities of both hips; left hip movement was flexion 100°, extension 20°, external rotation 40°, internal rotation 10°, abduction 30°, and adduction 20°. On the right side, full range of motion with mild pain was observed. The neurovascular examination showed normal result of both lower extremities. Laboratory examinations including hematology, biochemistry, coagulation, c-reactive protein, calcium, phosporus and alkali phosphatase resulted in normal value. Also, there was no habitual dietary abnormality that could induce osteoporosis.
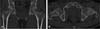
Plain anteroposterior pelvic radiograph showed inferomedial subcapital sclerotic changes on both side with small cystic lesion on left side (Fig. 1). Right and left hip lateral views showed minute sclerotic changes along subcapital area with small cystic lesion (herniation pit) on anterior area of left femoral neck (Fig. 2). Femoral alpha angle was 57.2° and 59.7° on the right and left side, respectively. Computed tomography image was obtained, but unfortunately any clear fracture line was not showed (Fig. 3).
T1-weighted magnetic resonance imaging (MRI) confirmed clear fracture line at infero-medial subcapital area around at both femoral neck. T2-weighted image revealed hyperintensity around both fracture line (Fig. 4). Bone mineral density examination resulted in normal findings. Total hip bone mineral density was 0.864 (T-score, –0.6; Z-score, 1.5). This result confirmed that the fracture was not due to the bone insufficiency condition.
The patient was treated conservatively and advised to take rest, use walking aids to avoid full weight-bearing and take non-steroidal anti-inflammatory drugs for pain control. One month later all symptoms was relieved and left hip range of motion was regained. We adviced the patient to reduce the magnitude of his work. Finally, the patient can return to his work after one month rest and he reduced his work burden. The patient has no complaint on further 5 months follow-up.
DISCUSSION
The clinical diagnosis of stress fracture is difficult, the symptoms often subtle and non-specific6) or even asymptomatic2). In our presented case, patient came only with unilateral left hip symptoms and no symptoms on the right side. Even there was some sclerotic appearance of right femoral neck at plain radiograph, right femoral neck stress fracture diagnosis was confirmed after MRI. We did not perform bone scintigraphy in this patient. Eventhough, it is a more sensitive and cost effective modality than MRI. We found a herniation pit on left subcapital area, this finding indicate that femoroacetabular impingement can be occured on the left side previously. This also supported by the higher alpha angle on the left side. This maybe associated with the presence of the symptoms on left side. A study on radiographic features of femoroacetabular impingement in femoral neck stress fracture patient has been performed previously7). Out of total 24 patients, cam morphology was seen in 6 patients (25.0%). Pincer morphology was seen in 14 patients (58.3%). Features of combined pincer and cam impingement was seen in 4 patients (16.7%). This study showed higher incidence of pincer type morphology, however its role as risk factor for femoral neck stress fracture remains unclear.
Our reported stress fracture involved an uncommon occupation that has never been reported previously. Only few cases associated with specific occupation has been reported. Similiar to our presented case, one of them associated with heavy lifting, which was bilateral femoral neck stress fracture occur in a male young adult stone mason and the symptoms was present on both side8).
The other case was in an adult woman who had bilateral symptomatic femoral neck stress fracture with history of long distance walking on her job9). The other rare hip stress fracture that associated with specific occupation was a unilateral trochanteric stress fracture involved a women window cleaner that commonly jumping during work10).
Our presented case was a bilateral femoral neck stress fracture in a shipman laborer which associated with history of heavy lifting during work. From this case, we learnt that stress fracture sometimes occur in an unexpected population and consideration of bilateral involvement is highly important in managing all suspected stress fracture case.



 XML Download
XML Download