

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Although the intramedullary nailing of subtrochanteric fractures of the femur is the current treatment of choice, this technique is limited by technical difficulties, postoperative peritrochanteric pain, and limping due to injury to the abductor muscles. In particular, intramedullary nailing in patients with multiple trauma including lung injury may adversely affect systemic physiology, the so-called “second hit” phenomenon. Moreover, this technique has been shown to be associated with the development of fat embolism and adult respiratory distress syndrome (ARDS), both of which can be fatal12). Therefore, special care should be taken to avoid fatal complications following surgical treatment for subtrochanteric fracture of the femur, especially in patients with multiple trauma including lung injury345).
The less invasive stabilization system-distal femur (LISS-DF; Synthes, West Chester, PA, USA) and the newly designed locking compression plate-distal femur (LCP-DF, Synthes) based on “minimally invasive surgery” have been developed for the treatment of distal femur fractures6). Plating techniques allow callus formation by percutaneous insertion and indirect reduction techniques, termed biologic plating, which maintains the vascularity of fragments with high stability. In particular, biologic plating is expected to have safe utility in patients with multiple trauma including lung injury, as the procedure does not require intramedullary reaming during the operation.
We hypothesized that surgical treatment using reversed contralateral application of LCP-DF and a minimally invasive technique represents an alternative method of stabilizing subtrochanteric fracture of the femur. Moreover, we anticipated that this procedure would have no adverse effect on postoperative pulmonary function regardless of the injury severity score (ISS) and surgical timing after injury, despite not performing damage-control orthopedic surgery at the time of injury. Accordingly, the aim of the present study was to evaluate the surgical outcomes of biologic plating using LCP-DF in patients with subtrochanteric fracture of the femur.
Go to : 
MATERIALS AND METHODS
1. Study Population
Between January 2010 and December 2013, 28 consecutive patients with subtrochanteric fractures of the femur treated with biologic fixation using LCP-DF were enrolled. Subtrochanteric fractures included 31A3, 32A, 32B, and 32C of the AO classification occurring between the lesser trochanter and the isthmus of the femoral canal. Exclusion criteria were patients with an open fracture, pathologic fracture, and atypical femoral fracture associated with the use of bisphosphonates. Preoperative values, including patient age, sex, affected side, fracture type, ISS, body mass index (BMI), surgical timing from injury to surgery, and type of lung injury were evaluated retrospectively. Multiple trauma was defined in the present study as injury including at least 2 different body regions with an ISS >15.
2. Surgical Technique
All operations were conducted with patients in the supine position on a fracture table with traction under general or spinal anesthesia. In order to achieve rotational alignment of the femur, central or slightly medial positioning of the patella was confirmed using C-arm preoperatively. Then, closed reduction was performed under fluoroscopic examination in the anteroposterior (AP) and lateral, and Lorenz views of the proximal femur.
In the majority of cases, it was difficult to achieve adequate closed reduction of flexed, external rotated, and abducted proximal fragments using traction on the fracture table only. Thus, indirect reduction techniques using various instruments, including long Kelly, Hoffman retractor, co-linear clamp, and percutaneous wire passers, were performed to reduce displaced proximal fragments in all cases. A 5 cm longitudinal incision was made distally from the vastus ridge. After splitting the iliotibial band, a Kelly or Hoffman retractor was inserted anterior to the proximal femur for reduction of flexion and external rotation of the proximal fragment. If the fractures were found to have a long spiral or oblique fracture line, a minimal incision was made at the level of the fracture to allow insertion of a co-linear clamp or a percutaneous wire passer for temporary wiring and reduction of the fracture (Fig. 1). Then, the vastus lateralis muscle was split in line with the fiber and an LCP-DF was introduced through the incision and advanced distally along the axis of the femur in the submuscular plane. In order to adhere the LCP-DF to the lateral cortex of the proximal femur, a 4.5 mm cortical screw was initially inserted, followed by the insertion of locking screws to fix the proximal fragment of the fracture. Finally, the distal part of the fracture was fixed with the insertion of locking screws. At least 4 locking screws were used to stabilize the distal part of the fracture (Fig. 2). At the end of the procedure, a drain was inserted and closure was performed in layers.
 | Fig. 1Closed reduction based on the minimally invasive technique under fluoroscopic examination. (A, B) Hoffman retractor placing for the reduction of flexion and external rotation deformity of the proximal fragment. (C, D) Temporary wiring using a percutaneous wire passer.
|
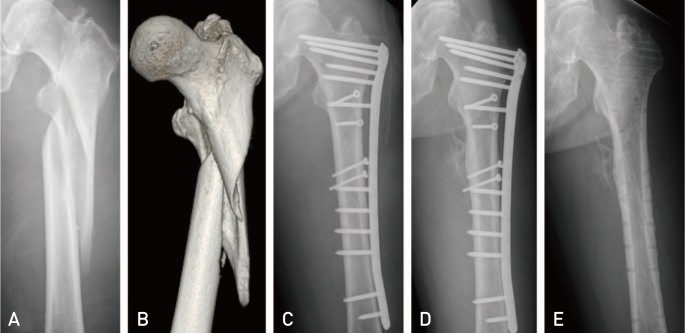 | Fig. 2(A, B) A 62-year-old patient with a complex subtrochanteric fracture after pedestrian accident. (C) Postoperative radiography after fixation with an locking compression plate-distal femur. (D) Fracture union at one year after fixation. (E) Radiography at the last follow-up visit after implant removal.
|
3. Postoperative Rehabilitation
All patients were encouraged to perform quadriceps strengthening exercises and straight leg-raising exercises postoperatively. After removal of the drain at 48 hours postoperatively, passive knee and hip range of motion exercises were initiated. Partial weight bearing using crutches was allowed as tolerated for the first 6 weeks, and weight bearing was gradually increased based on evidence of callus formation on follow-up radiography.
4. Radiologic Assessment
All patients were followed-up at 1, 3, 6, and 12 months, and then annually after primary surgery for clinical and radiographic evaluations of the fracture healing process. Radiologic assessments were evaluated using femur AP and lateral images of the affected side and hip AP, lateral, and Lorenz images of the proximal femur. Fracture union was confirmed by two orthopedic surgeons. Union was defined as full painless weight bearing with bridging callus across at least three cortices on AP and lateral views of the femur7). Nonunion was defined as a definite fracture gap after a minimum of 9 months from injury with no visible progressive signs of healing for 3 months.
Coronal alignment of the femur was evaluated postoperatively. Shortening of the femur was measured by orthoroentgenography during follow-up. External rotation deformity of the proximal fragment was assessed according to the configuration of the lesser trochanter and location of the patellar within the knee joint on the coronal plane. Complications such as implant breakage and screw breakage were recorded.
5. Clinical Assessment
Operative duration and intraoperative blood loss were recorded. Operative time was defined as the time from skin incision to the end of skin closure. Intraoperative blood loss was analyzed based on the estimated blood loss recorded by the anesthesiologist, which was the approximate amount of blood lost during the surgery. Fat embolism, ARDS, and infection during the follow-up period, and walking ability at the last follow-up visit were assessed using medical records. Clinical outcomes at the last follow-up visit were evaluated using the modified Merle d'Aubigne scoring system.
Go to :
RESULTS
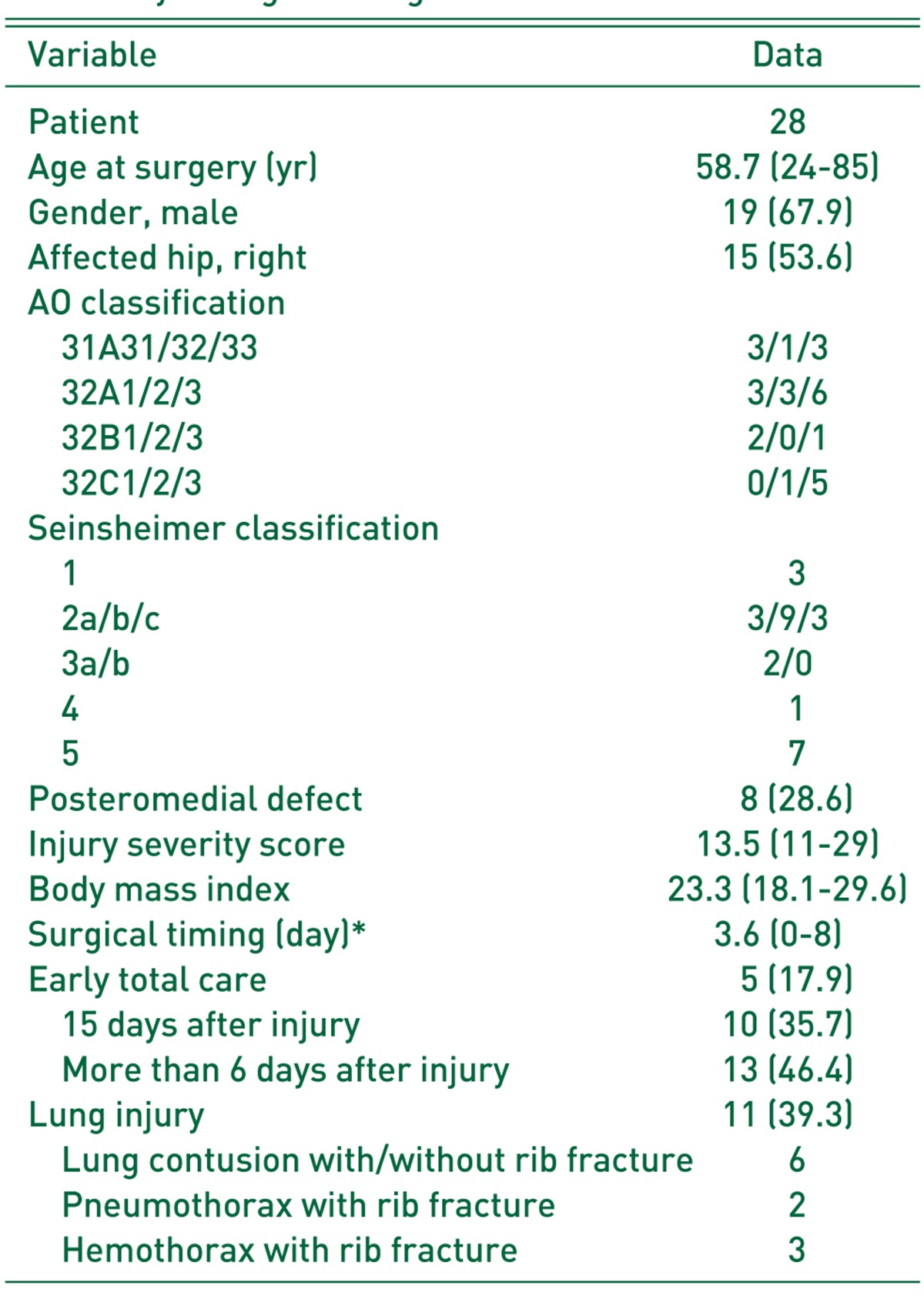
Patient baseline characteristics are provided in Table 1. The present study included 19 males and 9 females. The mean age was 58.7 years (range, 24-85 years). The right femur was involved in 15 patients and the left femur was involoved in 13 patients. Types of fracture according to the AO classification were 7 of type 31A3, 12 of type 32A, 3 of type 32B, and 6 of type 32C. According to the Sheinsheimer classification, there were 3 of type 1, 15 of type 2, 2 of type 3, 1 of type 4, and 7 of type 5. Of these, 8 patients (28.6%) had posteromedial defects. The mean ISS was 13.5 (range, 11-29), the mean BMI was 23.3 (range, 18.1-29.6), and the mean surgical timing (time from injury to surgery) was 3.6 days (range, 0-8 days). In the present study, 5 patients received early total care on the day of injury, 10 patients underwent operative treatment 1-5 days after injury, and 13 patients were operated on more than 6 days after injury. The ISS in all patients who had early total care was over 16. These patients required emergency operations, such as chest surgery or abdominal surgery, and fixation of the femur was performed on the same day under a single period of anesthesia.
The perioperative and postoperative outcomes of biologic fixation using LCP-DF in 28 cases of subtrochanteric fractures are provided in Table 2. The mean follow-up period of the 28 patients in the present study was 18.2 months (range, 14-43 months). The average operative duration was 88.1 minutes (range, 60-150 minutes) and the average intraoperative blood loss was 392.6 mL (range, 100-900 mL). The mean postoperative coronal alignment of the femur was valgus 1.2° (range, valgus 6.5° to varus 9°), and the mean shortening of the femur at the last follow-up visit was 0.3 cm (range, 0-1 cm). No patient had a varus or valgus malunion greater than 10°
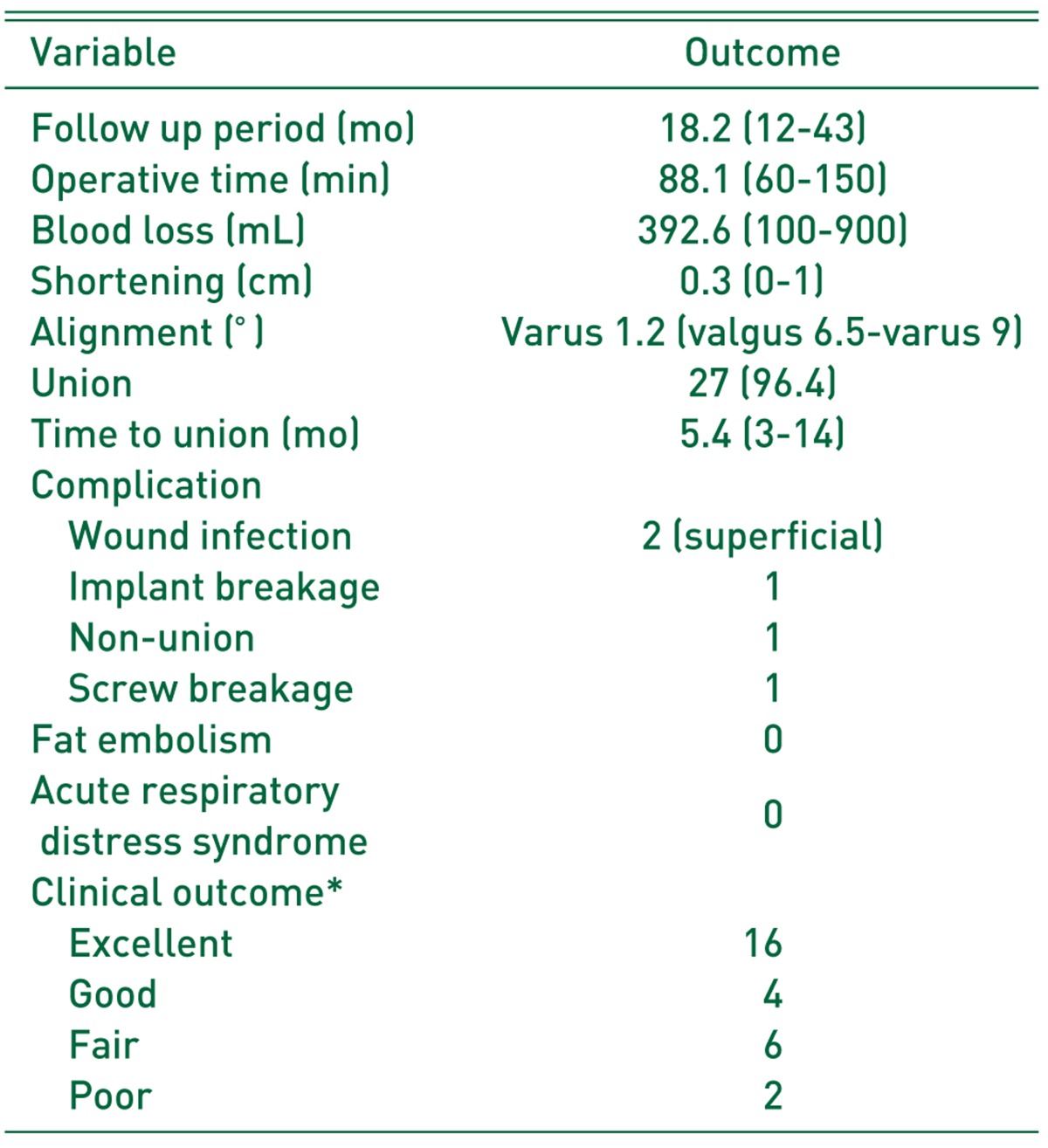
Fat embolism and ARDS were not observed postoperatively during the hospitalization period of the present study. Union was achieved in 27 patients (96.4%) after an average duration of 5.4 months (range, 3-14 months). There was 1 case of nonunion with implant breakage, 2 cases of superficial wound infection, and 1 case of distal locking screw breakage during the follow-up period. Modified Merle d'Aubigne scores at the last follow-up were excellent in 16, good in 4, fair in 6, and poor in 2 patients (Table 2).
Go to :
DISCUSSION
The purpose of the present study was to determine the radiologic and clinical outcomes of biologic plating using LCP-DF for the treatment of subtrochanteric fractures of the femur. In this study, fracture unions was achieved in 27 of 28 patients (96.4%) without any complications such as fat embolism or ARDS after surgery regardless of ISS, time from injury to surgery, and presence of lung injury.
Subtrochanteric fractures of the femur constitute 7% to 34% of proximal femoral fractures. This type of fracture typically occurs in active, young individuals due to high energy injury and is often accompanied by multiple injuries, including lung, brain, and abdominal injuries89). The predominantly cortical nature of the region, along with the strong muscular attachments and high compressive forces acting medially is responsible for intra-operative difficulties and the high rate of complications associated with the fractures of this region. The incidence of implant failure in patients with subtrochanteric fracture of the femur has been reported as high as 26%101112).
Intramedullary nailing has been wildly accepted as a representative surgical option for the treatment of subtrochanteric fracture of the femur. Theoretically, this surgical technique has a number of biomechanical advantages, including a shorter moment arm, greater strength, greater torsional stiffness, and greater load-sharing capacity, compared to plating technique1314). In particular, intramedullary nailing is based on the concept of relative biologic fixation, which preserves the vascularity of bone fragment, thereby minimizing soft tissue dissection and blood loss, compared to the traditional open-plating technique1516). Nevertheless, intramedullary nailing may provoke fat embolism or additional damage, the so called “second hit” which may cause ARDS postoperatively in patients with multiple trauma, including lung injury, due to intramedullary reaming during the procedure. Although there is controversy regarding the effect of intramedullary nailing on postoperative pulmonary function, the incidence of postoperative pulmonary complications including ARDS, pulmonary dysfunction, fat emboli, pulmonary embolism, and pneumonia have been estimated to be 4% to 38% among patients with femoral fractures in the presence of multiple injuries17). In particular, the incidence of postoperative ARDS has been reported as 2% to 15% after intramedullary nailing for the treatment of femur fracture1819). For this reason, the use of intramedullary nailing for the treatment of subtrochanteric fracture is limited in such cases.
On the other hand, extramedullary implants, such as dynamic hip screws, dynamic condylar screws, and angled blade plates, have been reported to have a strong association with secondary varus collapse, cutout, implant failure, and limb shortening on weight bearing. In particular, conventional methods of open plating with anatomical reduction and rigid fixation are reportedly associated with increased risk of nonunion, infection, implant failure, and re-operation due to extensive exposure, soft tissue stripping leading to devitalization of fragments, and loss of fracture hematoma2021).
However, Celebi et al.22) reported a 100% rate of fracture union in 33 subtrochanteric fractures after indirect reduction and biologic internal fixation using dynamic hip screws or angled blade plates. Vaidya et al.23) also reported that union was achieved in all cases (100%) after biologic plating using a dynamic condylar screw. They posited that the use of biological (indirect) reduction techniques instead of anatomic, open reduction was effective, particularly in comminuted subtrochanteric fractures. Based on these results, we hypothesized that biologic plating with minimally invasive surgery, which preserves blood supply around the fracture site, allows good surgical outcomes in patients with subtrochanteric fracture of the femur.
LCP-DF (Synthes) is an anatomical plate used in minimally invasive surgery and similar to the LISS-DF designed to fix distal femoral fractures. Although aiming devices are not currently available in Korea, plates can be inserted after the assembly of guide sleeves for locking screws onto plate under minimal incision, and locking screws can be fixed through the guide sleeve. In addition, LCP-DF appears to be suitable for biologic plating using minimally invasive surgery in patients with subtrochanteric fractures as greater biomechanical stability against axial loading has been reported24252627).
Acklin et al.28) reported bony union in 10 of the 14 cases of complex proximal femoral fracture (31A3) treated with indirect reduction and LISS-DF in a reversed contralateral application. In their study, 2 patients were lost to follow up, and 2 developed implant failure with early screw breakage and instability requiring re-operation. Oh et al.25) reported very good surgical outcomes after minimally invasive plate osteosynthesis (MIPO) of subtrochanteric femur fractures with a locking plate, with all patients healing without bone grafts in a mean time of 20.1 weeks. The authors posited that the use of the MIPO technique with a locking compression plate provides an alternative method for fixing subtrochanteic femur fractures in cases where IM nailing is deemed inappropriate.
In the present study, 27 patients healed without re-operation in a mean time of 5.4 months (range, 3-14 months). One patient who had nonunion with implant breakage required re-operation using intramedullary nailing. On retrospective evaluation of serial radiographs, we determined that the postoperative reduction of the fracture in this patient was not acceptable. The proximal fragment of the fracture was fixed on flexion and external rotation, and anterior cortical opposition was not achieved postoperatively. Lateral displacement of the proximal fragment was also identified. We posited that malreduction of the fracture may have increased stresses on the implant and fracture site (Fig. 3). Biomechanical studies have demonstrated that the integrity of the posteromedial trochanteric region is crucial in preventing implant failure after osteosynthesis of the proximal femur2930). Due to the greater tensile strains after osteosynthesis using LCP-DF, accurate medial buttressing to reduce the risk of healing complication is of particular importance (Fig. 4). It may be easier to reduce displaced proximal fragments in subtrochanteric fractures using biologic plating rather than intramedullary nailing. In addition, large posteromedial fragments can be fixed with lag screws when using biologic plating. However, we do not recommend the use of biologic fixation when reduction of the proximal fragment is not acceptable or sufficient restoration of large posteromedial defects is not possible.
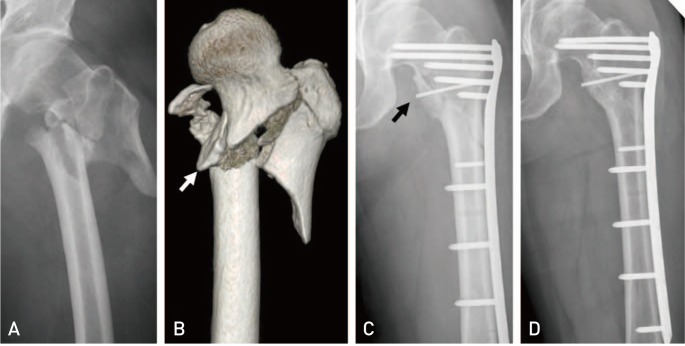
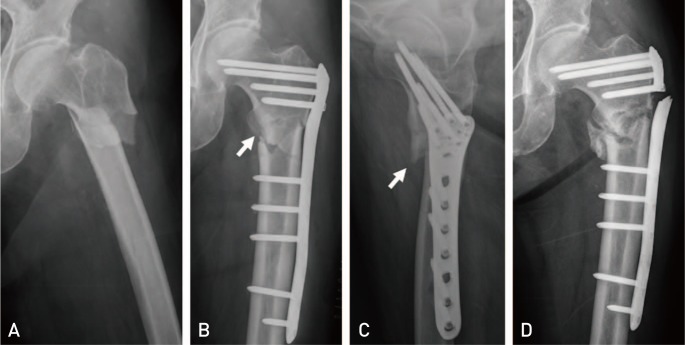 | Fig. 3(A) A 43-year-old patient with a 31A32 fracture of the proximal femur after falling accident. (B) Postoperative radiography demonstrated slight lateral displacement of the proximal fragment (arrow). (C) Lorenz image showing failure of anterior cortical opposition due to a flexion and external rotation deformity (arrow). (D) Radiography at one-year follow-up demonstrating nonunion of the fracture site with implant breakage.
|
The absence of any case of pulmonary function exacerbations postoperatively in the present study is encouraging. In total, 5 patients received early total care on the day of injury, 10 patients underwent operations within 5 days of injury, and none of the 11 patients who had lung injury developed any pulmonary complications such as fat embolism or ARDS after surgery. Oh et al.25) included 9 subtrochanteric fractures with various chest trauma. They reported that no cases of pulmonary exacerbation were identified postoperatively, although they did not report surgical timing from injury to operation. Based on these results, they posited that the MIPO procedure with an LCP is a safe surgical option in certain situations where nailing is not deemed appropriate.
Many recent studies have recommended damage control orthopedic surgery as an appropriate surgical approach to avoid worsening of patient condition due to the “second hit” of a major orthopedic procedure12). A recent prospective study reported that patients with multiple trauma subjected to secondary definitive surgery between days 2 and 4 had a significantly (P<0.0001) increased inflammatory response compared to between days 6 and 831). This finding indicates that it is safer to perform osteosynthesis for subtrochanteric fractures at least 6 days after injury in patients with multiple trauma. However, we were unable to identify the incidental difference in pulmonary complications postoperatively between patients who received early total care on the day of injury and patients who had operations within 5 days of the injury. Despite the small number of cases in the present study limiting the power of statistical analyzes, we suggest that biologic plating using an LCP-DF is a good surgical option for subtrochanteric fractures regardless of injury severity, surgical timing, and presence of lung injury.
There are limitations to the present study including a small cohort size, noncomparative design, retrospective study, and lack of statistical verification. In particular, we were not able to assess in changes of systemic inflammation and hypoxic damage after biologic plating by measuring important inflammatory mediators including interleukins, tumor necrosis factor, interferons, and colony stimulating factors. Moreover, we were not able to demonstrate the clinical effect of posteromedial defect in biologic plating due to the small sample size of the present study. Further studies with larger sample size are required to prove the role of posteromedial restoration in biologic plating. Finally, the LCP-DF was not developed for stabilization of the proximal femur.
Nonetheless, the findings of the present study demonstrate that biologic fixation using LCP-DF has a high success rate of fracture union with a low rate of radiologic complications and a low risk of pulmonary complications postoperatively regardless of injury severity, surgical timing, and presence of lung injury.
Go to :
CONCLUSION
Biologic fixation using locking compression plates may represent a good option in patients with subtrochanteric fracture regardless of injury severity, surgical timing, and fracture type. However, acceptable reduction with accurate posteromedial buttressing of the proximal fragment is essential to achieve satisfactory outcomes.
Go to :
 XML Download
XML Download