

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
High rates of morbidity and mortality are associated with hip fractures in elderly patients with underlying internal diseases and weakened systemic condition1). In particular, patients with kidney function failure frequently experience accompanied heart failure, anemia, malnutrition and other systemic weaknesses, and these conditions are risk factors that may induce adverse outcomes in fracture healing and patient recovery2). The incidence of hip fractures is higher in patients with renal failure than those without3), and morbidity and mortality rates after hip fractures are also reported to be higher45). Coco and Rush6) found that hemodialysis patients have 17.4 and 2.4 times higher incidence rates of hip fracture than non-hemodialysis patients, respectively.
Previous studies on hip fracture patients associated with renal failure mainly reported the clinical outcome of surgical treatment for femoral neck fractures. Patients with renal failure had a higher rate of morbidities such as non-union and osteonecrosis compared to those without after internal fixation of femoral neck fractures78). Comparative studies have been conducted to explore clinical outcomes after hip hemiarthroplasty49). However, no studies have been done to examine the results of internal fixation for intertrochanteric fractures.
This study aimed to compare clinical results and complications (e.g., non-union, osteonecrosis, hematoma, a failure of internal fixation, etc.) between hemodialysis patients and healthy individuals after undergoing proximal femoral intramedullary nailing for intertrochanteric fractures of the femur.
Go to : 
MATERIALS AND METHODS
1. Inclusion Criteria
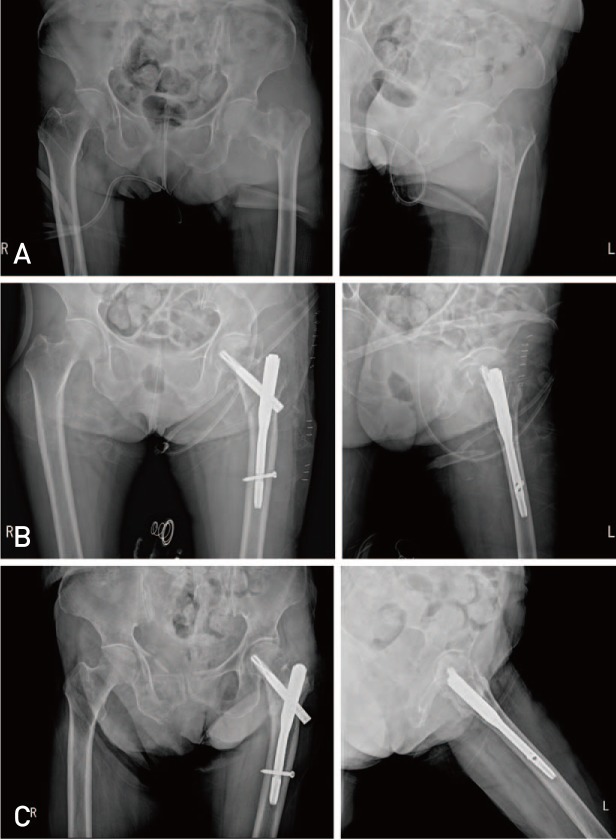
This study involved 47 patients who underwent internal fixation with the proximal femoral nail (PFN) for management of intertrochanteric femoral fractures between 2009 and 2014. These patients were devided into two groups: i) 17 in the hemodialysis group with end-stage renal disease, and ii) 30 in the control group with normal kidney function; clinical and radiological results were compared between the two groups (Fig. 1).
Initially, 87 patients having chronic kidney disease associated with a hip fracture were reviewed. Of these, 5 categorized as nonfunctional ambulators with a pre-fracture Koval score of 7 were excluded from the study. In addition, we excluded 51 cases without hemodialysis, 2 with peritoneal dialysis, 2 with pathological fracture, 3 with internal fixation using other than intramedullary nailing, 5 with hip hemiarthroplasty and 2 with kidney transplantation. Consequently, the hemodialysis group consisted of 17 patients without administration of immunosuppressive drugs or prednisolone.
2. Operative Methods and Postoperative Management
All operations were performed under general anesthesia or spinal anesthesia on the fracture table. Patients received closed reduction with adequate traction and rotation or invasive reduction through a small incision at the superior to the great trochanter. Accuracy of reduction was confirmed using fluoroscopy as measured by the maintenance of the reduction. A femoral nail was inserted and lag screw fixation was conducted from the posterior or posteroinferior to the proximal fragment. After fixation of the lag screw, the fixing screw was inserted to the distal femoral stem by loosening traction, in order to reduce a gap on the fracture site. Satisfactory fixation was obtained in all cases. A 200-mL drainage catheter was inserted to the great trochanter after placement of the nail cap.
Patients were allowed to sit as early as the first postoperative day and partial weight bearing ambulation was carried out over the first 6 weeks after surgery in the context of the patient's systemic condition. Patients started full weight bearing ambulation after improvement in health status and radiographic fracture union. Prophylactic antibiotics were administered preoperatively and intravenous antibiotics were injected until the 5th postoperative day.
3. Patient Demographics
Patient's gender, age, weight, height, bone mineral density (BMD; lumbar spine and femoral neck) and associated underlying diseases were examined. Duration of hemodialysis treatment, pre- and postoperative blood test results (hemoglobin [Hb], hematocrit [Hct], platelet, prothrombin time [PT]/activated partial thromboplastin time [aPTT]), operation time, intra-operative blood loss, postoperative drainage and transfusion and others were examined in the hemodialysis group. Intraoperative blood loss was measured by calculating the difference between irrigation volume and drain volume and the number of gauzes used during the surgery. All operations were performed by the same medical team using the same surgical technique. For objective interpretation, radiological and clinical outcomes were analyzed independently by two orthopedic surgeons.
Based on preoperative radiographic findings, fracture types were classified as stable or unstable fractures according to the number of bone fragments and the degree of calcar displacement10). To determine whether postoperative stability of fixation was achieved, we checked reduction inside the cortical bone area on anteroposterior and lateral radiographic views (postoperative hip anteroposterior, axial X-ray) and location of the lag screw placed at the inferior or posteroinferior aspect of the proximal fragment. Furthermore, the degree of reduction was assessed according to neck-shaft angle and evaluated as good (<5° of angulation), acceptable (5-10° of angulation) and poor (>10° of angulation), and tip-apex distance (TAD) was measured1112). Patient's pre- and postoperative ambulatory ability was evaluated using the Koval classification13).
Plain radiography was taken every two weeks for the first month after surgery and at the 1-month check-up afterward on an outpatient basis. Fracture union was defined as the formation of cortical callus bridge in at least 3 cortices and no fracture line visible on anteroposterior and lateral radiographic views without pain during weight bearing. Non-union was defined as the absence of the above healing responses for more than 6 months after surgery14). Patients were examined during the postoperative period, and complications were identified including hematoma requiring drainage for more than 4 days, deep vein thrombosis, infection, iatrogenic nerve injury, osteonecrosis and revision surgery. In addition, mortality rates within or after the first postoperative year were determined.
4. Statistical Methods
Radiological and clinical outcomes between the hemodialysis and control groups were compared using paired t-test and chi-square test. Binominal logistic regression analysis was performed to analyze the effect of hemodialysis on postoperative ambulatory status. Statistical analyses were conducted using PASW Statistics ver. 18.0 (IBM Co., Armonk, NY, USA).
Go to :
RESULTS
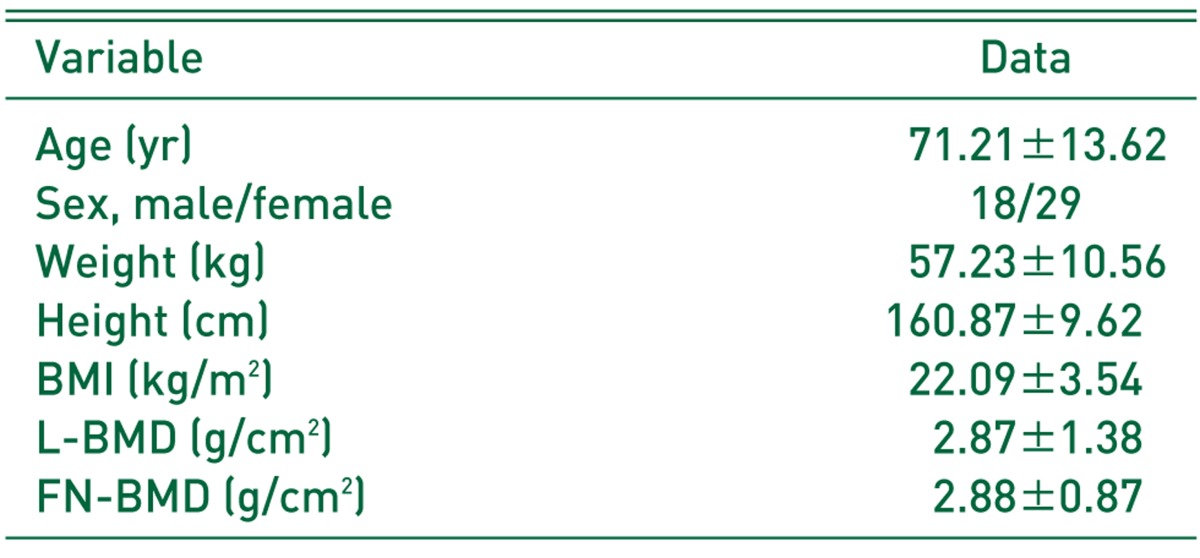
A total of 47 patients were included and their age was 71.21±13.62 years (mean±standard deviation). Body weight was 57.23±10.56 kg, and height was 160.87±9.62 cm. The body mass index (BMI) was 22.09±3.54 kg/m2, and BMD was 2.87±1.38 g/cm2 in the lumbar spine and −2.88±0.87 in the femoral neck. The subjects were 18 males and 29 females. A total of 47 fractures were included (16 cases of right-side fracture and 31 cases of left-side fracture). The cause of fractures was fall occurred during walking or moving in all cases (Table 1).
1. Clinical Results
Underlying internal diseases associated were hypertension, diabetes mellitus, cerebrovascular disease, lumbar spinal stenosis, hyperlipidemia, cardiac failure, a history of myocardial infarction, respiratory disease and others. Of these, conditions appeared to be directly linked to ambulation were cerebrovascular disease in 3 cases (pre-operative Koval scores of 1, 3 and 5, respectively) and lumbar spinal stenosis in 1 case (pre-operative Koval score of 1). However, no difference was found between preoperative and postoperative bilateral muscular strength in both lower and upper extremities.
The duration of hemodialysis was 5.8±3.2 years (mean±standard deviation) in the hemodialysis group, and the follow-up period was 29±16.1 months. There was no significant difference in age, weight, height and BMI between the hemodialysis group and the control group. Moreover, no significant difference was found in gender, fractured side (right/left) and incidence of unstable fractures between the two groups (Table 2).
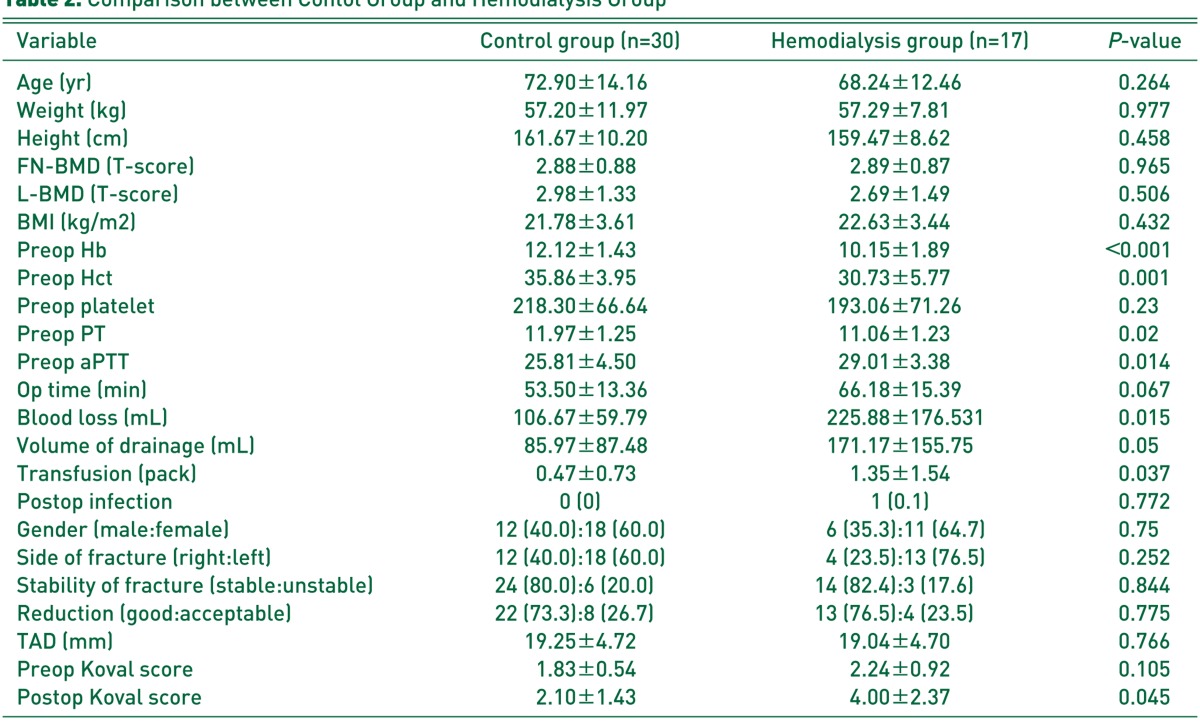
Table 2
Comparison between Contol Group and Hemodialysis Group
Values are presented as mean±standard deviation or number (%).
BMD: bone mineral density, FN: femoral neck, L: lumbar spine, BMI, body mass index, Hb: hemoglobin, Hct: hematocrit, PT: prothrombin time, aPTT: activated partial thromboplastin time, Preop: preoperative; Op: operation, Postop: postoperative, TAD: tip to apex distance.
![]()
The operation time was 66.18±15.39 minutes in the hemodialysis group and 53.50±13.36 minutes in the control group. Although the operation time was slightly longer in the hemodialysis group, there was no statistical significance (P=0.067). The intraoperative blood loss was 225.88±176.53 mL in the hemodialysis group, showing a significantly larger blood loss volume compared to 106.67±59.79 mL in the control group (P=0.015). The postoperative drainage volume was 171.17±155.75 mL in the hemodialysis group, having a significantly larger amount compared to 85.97±87.48 mL in the control group (P=0.05). The postoperative transfusion was 1.35±1.54 pack in the hemodialysis group, exhibiting a significantly higher volume compared to 0.47±0.73 pack in the control group (P=0.037) (Table 2).
Preoperative Hb/Hct was 10.15±1.89/30.73±5.77 in the hemodialysis group and 12.12±1.43/35.86±3.95 in the control group, which was significantly lower in the hemodialysis group. PT/PTT was 11.06±1.23/29.01±3.38 in the hemodialysis group and 11.97±1.25/25.81±4.50 in the control group, demonstrating significant extension (P=0.014). Platelet was 193.06±71.26 in the hemodialysis group and 218.30±66.64 in the control group, but had no statistical significance (P=0.23). With respect to postoperative infection, non-union associated with infection occurred only in 1 cases of the hemodialysis group, showing no statistical significance (P=0.772) (Table 2).
2. Radiological Results
Postoperative reduction status of the fracture site was good in 13 cases (76.5%) and acceptable in 4 (23.5%) in the hemodialysis group, and good in 22 cases (73.3%) and acceptable in 8 (26.7%) in the control group. There was no patient with poor reduction in either group and no statistically significant difference was found between the two groups (P=0.775). TAD was 19.04±4.70 mm in the hemodialysis group and 19.25±4.72 mm in the control group, showing no statistically significant difference (P=0.766) (Table 2).
Fracture union was achieved in most patients after surgery in both groups, but there was 1 case with non-union associated with infection in the hemodialysis group. This patient received additional surgical management for infection and was mobile only via a wheelchair due to nonfunctional ambulation. In addition, a patient died within one year after surgery.
A patient in the control group had a failure of internal fixation on the 4th postoperative month, and alternatively managed with hip hemiarthroplasty. This patient was mobile only via a wheelchair due to nonfunctional ambulation. Another patient had a periprosthetic fracture of internal fixation devices 1 year and 4 months after surgery and underwent revision intramedullary nailing with long nails. This patient achieved bone union 4 months after revision and able to ambulate.
3. Ambulatory Status
The mean±standard deviation of Koval score was 2.24±0.92 in the hemodialysis group and 1.83±0.54 in the control group, exhibiting no significant difference in pre-fracture ambulatory status between the two groups (P=0.105). The postoperative Koval score was 4.00±2.37 in the hemodialysis group and 2.10±1.43 in the control group. The hemodialysis group had a significantly worse score than the control group (P=0.045) (Table 2).
The number of patients categorized as nonfunctional ambulation (grade 7) using a wheelchair was 7 (43.8%) out of 16, excluding a case of death among 17 patients in the hemodialysis group and 3 (10.0%) out of 30 cases in the control group. In binominal logistic regression analysis of gender, age, fracture instability, fracture orientation and other variables, the odds ratio of inability to walk after surgery was 13.48 times higher in the hemodialysis group (P=0.005; 95% confidence interval [CI], 2.166-83.912) (Table 3).

Go to :
DISCUSSION
This study investigated possible complications, non-union and postoperative ambulatory ability in hemodailysis patients who underwent internal fixation with PFN for management of intertrochanteric fractures of the femur by comparing with the control group (i.e., normal kidney function). Non-union is the most common complication following fracture fusion in patients with renal failure15). Bone healing and formation of new tissue are inhibited by osteoporosis and renal bone insufficiency occurring in patients with renal failure1617). The causes are vitamin D deficiency, calcium imbalance in the plasma, hyperparathyroidism, chronic acidosis and others1819). The incidence of non-union increases in hip fracture patients with end-stage renal failure due to amyloid deposition and aggravated renal bone insufficiency7). Nutritional deficiency associated in renal failure patients has negative effects, and this may lead to insufficient supply of energy, protein and carbohydrate necessary in cell movement, cell differentiation and formation of repairing tissues occurring during fracture healing process due to albumin excretion abnormality, lack of supply of essential nutrients, erythropoietin deficiency anemia and others20).
Kuo et al.15) reported that revision rates ranged between 30-46% after internal fixation of femoral neck fractures occurred in renal failure patients, and recommended renal impairment and the degree of fracture displacement as risk factors2122). Kalra et al.8) proposed that revision rates reached up to 83.3% because of increased rates of nonunion and osteonecrosis after internal fixation of femoral neck fractures in hemodialysis patients, and the revision rate was markedly higher than that of renal failure patients not undergoing hemodialysis (20-36%)23). The occurrence of non-union is reported to be 2% in intertrochanteric fracture patients without kidney disease2425).
In the current study, non-union associated with infection occurred in a patient after undergoing proximal femoral nailing for intertrochanteric fractures in the hemodialysis group, but no statistical significance was found. Unlike femoral neck fractures, this seems to be attributable to preservation of blood supply to the femoral head and a wider area of the fracture plane and more stable fixation than in the neck in intertrochanteric fractures.
In the present study, patients in the hemodialysis group presented with a variety of internal diseases and weakened systemic condition and had a lower pre-operative Hb and Hct and a significantly extended PTT compared to those in the control group. Extended PTT is thought to be attributed to heparin administration during hemodialysis. This hematological imbalance resulted in a significant increase in intraoperative blood loss, showing no statistical significance but, increased volume of blood loss appears to contribute to an extension of operation time. Eventually, this may have led to a significant increase in transfusion volume.
The correlation between hemodialysis duration and hip fracture incidence has not yet been clarified326). However, the low BMD in hemodialysis patients is known to be the most significant risk factor in the incidence of hip fractures27). Our study found no significant difference in BMD between the hemodialysis and control groups. Although not significant, the hemodialysis group was younger and had a higher BMI, and no consideration of a history of osteoporosis treatment seemed to act as a variable.
Koval et al.13) suggested that malnurished patients with hip fractures had a longer length of hospital stay and higher mortality rate and lower chance of recovery to pre-fracture level of physical activity. In this study, the hemodialysis group regarded to be associated with malnutrition20) had significantly poorer postoperative Koval scores than the control group and had 13.5 times higher risk of disability to walk by using a wheelchair after surgery (13.48; P=0.005; 95% CI, 2.166-83.912).
Karaeminogullari et al.4) addressed the 2-year mortality rate of 45% in a study on 29 hemodialysis patients with hip fractures. Schaab et al.28) reported that all of 6 renal failure patients with hip fractures died within one year without surgical treatment. Klein et al.29) recommended that the 1-year mortality rate was 38% in 8 hip fracture patients associated with end-stage renal disease, and collaborative interdisciplinary care with nephrologists and early ambulation are crucial in decreasing morbidity and mortality rates. The 1-year mortality rate is reported to range between 10-20% in patients with intertrochanteric fractures and normal kidney function. In our study, one patient died among 17 hemodialysis patients after proximal femoral nailing for treatment of intertrochanteric fractures.
Karaeminogullari et al.4) suggested that internal fixation needs to be taken into consideration as the primary option for hip fractures in hemodialysis patients excluding cases of displaced femoral neck fractures. In this study, non-union and other complications rarely occurred in patients who underwent intramedullary nailing for intertrochanteric fractures. Therefore, intramedullary nailing should be considered as the primary treatment option instead of primary hip hemiarthroplasty. However, additional studies are required to further compare postoperative ambulatory status and complications between intramedullary nailing and primary hip hemiarthroplasty.
This retrospective study was limited by no investigation of causes of hemodialysis in the experimental group and no assessement on pre- and postoperative systemic nutritional status. Moreover, this study was unable to statistically analyze all underlying internal diseases having a direct or indirect influence on ambulation, so complementary studies are thought to be warranted. This study was meaningful in that it revealed the clinical outcomes of proximal femoral nailing by involving a relatively large group of hemodialysis patients associated with intertrochanteric fractures.
Go to :
CONCLUSION
Hemodailysis patients who underwent proximal femoral nailing for intertrochanteric fractures of the hip had no significant difference in bone union and radiological results compared to the control group with normal kidney function. However, the risk of inability to walk after surgery was about 13.5 times higher in the hemodialysis group. Since hemodialysis patients are associated with more internal diseases and hemodynamically unstable pre- and postoperatively, they require special attention. For recovery to preoperative ambulatory status through accurate reduction, firm fixation and early ambulation, attentive postoperative rehabilitation is warranted.
Go to :
 XML Download
XML Download