

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Of all skeletal injuries, approximately 3% consist of pelvic fractures1). Especially in high energy trauma (HET), disruption of the pelvic ring occurs in approximately 13-17% of all pelvic fractures2). High forces are required to disrupt the pelvic ring and the association with other significant injuries is therefore high3). Mortality is reported to be as high as 10-16% in this patient group4). When there is an open fracture, mortality as frequent as 50% has been reported5). Significant hemorrhage is an often encountered complication seen in unstable pelvic ring injuries678). Because early exsanguination is the major cause of death in these patients, early identification of the bleeding source and rapid stabilization of the fracture are therefore critical in their survival9).
The exact treatment pathway of hemodynamically unstable patients with an unstable pelvic ring fracture remains controversial and is often dictated by available hospital facilities. Mortality and functional outcome of pelvic ring injuries are determined by several factors, especially concomitant injuries. The major factors influencing chronic disablities are urogenital and neurological injuries1011).
This study was conducted to evaluate the patient profile, fracture characteristics, treatment and outcome of a large patient group with various pelvic ring injuries in our clinic.
MATERIALS AND METHODS
A total of 537 patients with a pelvic fracture were admitted to our hospital (Radboud University Medical Centre in Nijmegen, the Netherlands) in the period January 1, 2004 to January 1, 2015. Our hospital is a level 1 trauma center and a supra-regional referral center for pelvic and acetabular fractures in the Netherlands. Also, it is the main referral center for the Dutch Helicopter Emergency Medical Service (HEMS) for the middle, east and south part of the Netherlands. After the approval from Institutional Review Board of Radboud University Medical Centre, all data were analyzed from the electronic patient charts and the trauma database. Data analyzed included patient demographics, date, cause and type of the accident, HEMS involvement, transfusion requirement, associated injuries, abbreviated injury scale for each body region, injury severity score (ISS), treatment in the emergency room (ER), length of intensive care unit (ICU) and hospital stay, complications and mortality. The pelvic fractures were described according to Tile's classification12). In our center, each patient with a pelvic fracture is routinely evaluated with a computed tomography scan. The specific fracture sites were also described. If operative therapy was performed, type of fixation, secondary operations and operation time were recorded.
Data of patients with an isolated acetabular fracture were excluded as well as data of patients who were referred for non-, or malunions of pelvic fractures.
During this 10-year period no significant changes in management or diagnostic work-up of pelvic fractures were made.
1. Statistical Analysis
Statistical analyses were performed using SPSS ver. 13.0 (SPSS Inc., Chicago, IL, USA). Mann-Whitney U-test was performed to establish significance between the numbers of days of admittance in both groups. Chisquare test was performed to determine significance in nonparametric variables.
RESULTS
Five hundred and thiry-seven patients had suffered pelvic fractures. There were 328 (61.1%) men and 209 (38.9%) woman. Mean age was 44 years (standard deviation, 18; range, 2-100 years). Age didn't differ significantly between men and women. There were 45 pediatric patients in the range from 2 to 17 years. The HEMS was involved on the place of accident in 200 patients (37.2%).
1. Cause of Accident
In the majority of cases (465/537; 86.6%), the pelvic injury was due to a HET. From the HET patients 302 (64.9%) were due to a road traffic accident, 121 (26.0%) to a fall from height and 42 (9.0%) to a crush accident. Seventy-two cases were due to a low energetic trauma, like a domestic fall.
2. Referral of Patients to Trauma Center
Four hundred and twenty-four patients (79.0%) were initially transported to a level 1 trauma center, most of them to our hospital. Nine patients (2.1%) were initially presented to a hospital abroad, this because of the function of our hospital as a level 1 trauma center for the part of Germany in the proximity of the border. These hospitals are all level 2 or 3 trauma center. All other patients (n=104, 19.4%) were stabilized in another hospital and transferred to our hospital later.
3. Classification
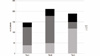
We encountered 137 Tile type A fracture (25.5%), 211 type B fractures (39.3%) and 189 type C fractures (35.2%) (Fig. 1). Of all type A fractures, the type of A1 was zero (0%), the type of A2 was 115 (83.9%) and the type of A3 was 22 (16.1%). Of the type B fractures, the type of B1 was 49 (23.2%), the type of B2 was 129 (61.1%) and the type of B3 was 33 (15.6%). Of the type C fractures, the type of C1 was 118 (62.4%), the type of C2 was 31 (16.4%) and the type of C3 was 40 (21.2%).
4. Presentation
Mean revised trauma score (RTS) was 11 (range, 3-13). Eighty-six patients had as RTS <10, which was mainly due to a low Glasgow coma scale score. The RTS didn't differ significantly among Tile A, B or C fractures.
Mean ISS was 26. Only 132/537 patients (24.6%) had an ISS <16. Mean ISS was significantly higher in more complex fracture types (33 in Tile C vs. 26 in Tile B vs. 19 in Tile A).
5. Shock Class
Mean shock class according to Advanced Trauma Life Support (ATLS®; Trauma Programs, Chicago, IL, USA)13) was 2. Of all patients, 256 (47.7%) were hemodynamically unstable (shock class 2 or higher) according to ATLS® when they arrived at the ER. Patients with a Tile C fracture were significantly more often hemodynamically unstable than patients with a Tile A or B fracture (68.2% vs. 38.4% vs. 34.1%, P<0.01). In total 205 patients (38.2%) received transfusion with packed red blood cells (PRBCs). Mean PRBC transfusion was 3.5 units (range, 1-30 units) within the first 24 hours after the accident. Mean PRBC transfusion was significantly higher in Tile C fractures compared to Tile A and B fractures (1,700 vs. 1,000 vs. 1,100 mL, P<0.04).
6. Concomitant Injuries
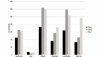
Concomitant injuries are shown in Fig. 2. Concomitant injuries were seen in 80.3% of the patients with a Tile A fracture, in 83.2% of the patients with a Tile B fracture and in 90.4% in patients with a Tile C fracture. Only 84 patients had an isolated pelvic ring fracture.
7. Open Pelvic Fractures
Twenty-seven patients had an open pelvic fracture (5.0%). Mean age was 33 years (range, 5-58 years), mean RTS was 11, mean ISS was 31, and mean shock class was 2. Patients with open fractures received a mean of 5 PRBCs (range, 0-28 PRBCs) within 24 hours after the accident. Except for the RTS, these findings were all significantly higher than patients with closed fractures.
Five patients had a grade 1 open injury (according to Gustilo and Anderson14)), 12 patients had a grade 2 open fracture, and 10 patients a grade 3 open injury. In this group, no traumatic hemipelvectomies were encountered.
8. Pre-hospital Stabilization and Stabilization in the ER
Pre-hospital stabilization was done with a T-POD® (Pyng Medical, Richmond, BC, Canada) or a pelvic sling in 2 patients with a Tile A fracture, 31 patients with a Tile B fracture and 54 patients with a Tile C fracture. Additional emergency stabilization was carried out on the ER in 5 patients with a Tile A fracture, 60 patients with a Tile B fracture and 103 patients with a Tile C fracture. Also in 2 patients with a Tile C fracture a pelvic C-clamp was applied in the ER.
9. Acute Stabilization
Acute stabilization of the different fracture types are listed in Table 1. Only one patient with a Tile A fracture was operatively stabilized because of severe dislocation. In Tile B fractures, 73.5% were not operatively stabilized in the acute phase. This is mainly due to the large number of type B2 fractures. In patients with a Tile C fracture, ORIF was conducted in 50.8% of the patients. This includes open plating as well as percutaneous screw placement (anterior and posterior). In 65.0% of these patients, only the anterior ring was stabilized as a damage control procedure. In the remaining group the anterior and posterior ring was stabilized (early total care). In 23 patients angiography with selective embolization was carried out as to stabilize the patient. A complex fracture type was seen in 15 of 23 patients (65.2%).
A laparotomy was done in 70 patients, of which in 50 patients (71.4%) this was a damage control laparotomy (DCL). DCL were distributed equally among the different fracture types. In 22 additional patients with a Tile C injury, the lesser pelvis was packed with gauzes without a formal laparotomy. In all other patients, bowel or diaphragm injuries were the reason for laparotomy.
10. Definitive Stabilization
In Tile A fractures, no further operative stabilizations were carried out. Definitive operative stabilization for Tile B and C fractures are listed in Table 2. Only 35.5% of the Tile B fractures was stabilized operatively. This is mainly due to the high percentage of Tile B2 fractures in our population (61.1%). In the Tile C group, definitive stabilization was done in 82.5% of the patients. Of the patients who weren't operated, many of them died before definitive care could be performed, or they were not fit for surgery due to infectious complications or severe head trauma. Fig. 3 demonstrate a typical case of a type C injury, plate fixation of the anterior ring initially and secondary sacroiliac (SI) screw placement.
11. Complications
Complications during admittance are listed in Table 3.
Urogenital injuries were seen in 8 patients; 3 patients with a Tile B and 5 patients with a Tile C fracture. Six patients had a urethral rupture. One patient had a severe open fracture with a penile laceration and one patient complained of erectile dysfunction during follow-up.
Neurologic injuries were seen in 20 patients. Seven patients were hemiplegic directly due to a vertebral fracture with spinal cord injury. Nerve palsies were seen in 13 patients. In 4 patients, this was a distal nerve palsy related to a fracture of the lower leg. Nerve palsy of the sciatic nerve or lumbosacral root was seen in 9 patients; 4 patients had a Tile B fracture, 5 patients a Tile C fracture.
12. Mortality
Overall mortality in our group was 13.6% (73/537). Mean ISS of diseased patients was 47 (range, 4-75). Forty-five in 73 patients (61.6%) received PRBCs. Twenty-eight patients that did not get transfusion were considered responders to volume replacement. The number of deaths remained the same over the years with a peak incidence in 2012 (Fig. 4).
Of the 73 patients that died, 20 patients had a Tile A, 21 a Tile B and 32 a Tile C fracture. Mortality was significant higher (P<0.05) for Tile C injuries compared with Tile B, but not for Tile A injuries.
Nineteen of 73 patients (26.0%) died within the first 24 hours after the accident. Nine of these patients (47.4%) died solely to severe head trauma. In 10 patients (52.6%), hemorrhagic shock contributed to, or was the cause of death. In all patients, the pelvic fracture contributed significantly to the hemorrhagic shock.
The other 54 patients died in a range of 2-59 days. Most of them died due to late sequelae of hemorrhagic shock or neurotrauma.
13. Length of Stay
Mean length of stay was 20 days. In total, 291 patients were admitted to the ICU (54.2%). Mean length of stay on the ICU was 5.5 days. Length of stay was significantly longer for patients with a Tile C injury than for patients with a Tile A or B injury. Length of stay on the ICU didn't differ significantly.
14. Destination after Discharge
Destination after discharge is listed in Table 4. Almost half of the patients could be discharged to their homes. Patients with stable fracture types could be discharged to home significantly more often than patients with unstable fracture types (P<0.03). An additional group of 19.9% were discharged to home after treatment in a rehabilitation clinic. The patients of 15.5% were transferred to other hospitals, mainly to a hospital closer to home.
15. Comparison Tile A vs. B vs. C
An overview of the different fracture types is given in Table 5. Patients with an unstable pelvic injury (Tile B1, B3, and C) presented with a significant higher ISS and shock class (P<0.02). Also, the rate of acute stabilization,the need for laparotomy and definitive operative stabilization was significantly higher in patients with an unstable fracture (P<0.04). Major complications were seen more often in patients with a Tile C fracture in comparison with a Tile A or B fracture (P<0.02). However, mortality between all groups didn't differ significantly.
Patients with a stable B2 fracture had a significantly lower ISS, shock class and stabilization rate than patients with an unstable fracture. Of all patients who were in need of operative stabilization of the fracture (n=222), 138 were managed in the acute phase (62.2%).
DISCUSSION
The patient data describe a consecutive patient series over a period of 10 years in a level 1 trauma center in the Netherlands and describes our experiances with pelvic fractures.
As shown by other authors114), pelvic fractures are predominantly seen in men less than 50 years of age and are involved in a HET of which most of them in a motor vehicle accident. These findings are similar to our patient group.
An explanation for the majority of HEMS involvement after 2006 can be explained by the fact that operating hours were extended to 24 hours a day and the criteria for HEMS involvement were broadened.
Tile A fractures are thought to be relatively benign because the stability of the pelvic ring remains intact and the risk of severe hemorrhage from the venous plexus is considered low15). However, in our group of patients with a Tile A fracture, almost 80% had concomitant injuries and had a relatively high ISS with a mean of 22. Also, almost 40% was hemodynamically unstable. Possible explanations can be that most patients with a simple fracture of the pubic ramus are not admitted and can be treated in the out-patient clinic with analgesics and physical therapy and therefore are not included in our analysis. This can bias our results. Also, in patients with an isolated iliac wing fractures, high energy impact is necessary to cause this type of fracture and a lot of concomitant injuries are seen in these patients. Therefore, this group of patients have similar patient profiles and outcomes as patients with unstable fractures have.
In the patient group with a Tile B-type fracture, also a high ISS was seen. Prehospitally, in only 31 patients (14.7%) a pelvic stabilization device was used. This might be related to the limited use of pelvic compression devices by the emergency medical team, unclear findings in physical examination or insufficient documentation of the paramedics or the ER department. Experience nowadays in our clinic is that in patients with the slightest suspicion of a pelvic fracture, a pelvic stabilization device is used. This subject is currently studied in a new prospective case series.
Early total care was done in 50.8% of the patients with an intrinsic unstable fracture with a shock class of 2 or lower. Most of these patients were treated with symphyseal plating alone. In hemodynamically unstable patients, damage control principles were followed; either an external fixator was placed or a symphyseal plate was used. When the patient was stabilized, a secondary procedure was performed with placing of SI screws. Plating of the symphysis is a fast and easy procedure and if the patient and the fracture allow it, we prefer this over the external fixator. The advantage of this approach is direct and often better reduction of the anterior ring without the complications of external fixation devices, such as pintract infections or non-adequate placement of pins. The posterior pelvis was often stabilized in a second procedure.
The patients with the Tile B2 type fracture were treated conservatively, because we believe that this type of fracture is intrinsic stable. However, one patient with a B2 fracture who could not mobilize due to extensive pain in the SI joint were stabilized later with percutaneous SI screws, with good result.
The majority of our patients had a Tile C fracture. Ninety percent of patients had concomitant injuries; therefore, the mean ISS was high. As expected the rate of major complications and mortality was the highest in the type C group. However, the number of urogenital and neurologic complications was considerably low, especially considering the amount of complex pelvic fracture patients included in this study.
Most complications seen were due to late effects of hemorrhage (systemic inflammatory response syndrome) and due to thoracic trauma (acute respiratory distress syndrome, pneumonia). Patients who had an open fracture suffered mostly from infectious complications.
The number of complications reported here is suspected to be higher than documented. This is especially true for the minor complications like electrolyte disturbances and urinary tract infections. Major complications requiring operative therapy or ICU admittance are well documented and are therefore believed to be accurate.
Mortality in our total group was 13.6%, which is acceptable in comparison with other studies141116). For example, Rommens and Hessmann16) report a mortality rate of 5% in the group with Tile B fractures and 14.8% in Tile C fractures. In this group also a lot of concomitant injuries were seen. Death due to hemorrhage shock was seen in 9 patients (40%) compared with 10 patients (52.6%) in our group. Mortality over the past 10 years didn't change. However, this study can be the basis for evaluating our protocol in order to reduce mortality even further.
Approximately 47% of all patients could be discharged to their homes with physical therapy and no further need for clinical rehabilitation. Outcome was therefore considered generally good. However, no functional outcome scores were measured during follow-up. Information regarding walking, pain and return to former jobs could only be found in a select number of patient-charts, so no conclusions can be made of this retrospective data. Evaluation of functional outcome with the 36-Item Short Form Survey (SF-36) and the Majeed questionnaire17) is currently being studied in a prospective trial.
CONCLUSION
This study, conducted in a trauma center in the Netherlands which is dedicated to the treatment of pelvic ring injuries, shows a high incidence of pelvic fractures. To our knowledge, this is the largest reported single centre experience in the Netherlands. Patients with a Tile C fracture are more severely injured and require more resources. Mortality doesn't differ between the 3 fracture types according to Tile. This is suggestive that mortality is caused by a variety of other injuries such as neurotrauma. The overall outcome is considered good with almost half of the patients can be discharged to their homes.
This data is an important tool to evaluate our treatment protocol and thereby improving outcome.







 XML Download
XML Download