

 PDF
PDF ePub
ePub Citation
Citation Print
Print


In recent years, proximal femoral nailing has become a primary surgical method for the treatment of intertrochanteric femoral fractures based on its mechanical advantages. However, this treatment requires the adduction and internal rotation of the injured limb of the patient for the insertion of the guide pin and the femoral nail. In addition, the perineal post, installed for traction, puts significant pressure on medial soft tissues further pressing toward the femur. Therefore, the blood vessels, traveling inside of the thigh, could be displaced and moved adjacent to the femur. In this report, we present the case of delayed diagnosis and management of a deep femoral artery rupture. This rupture occurred during the insertion of a distal interlocking screw with a proximal femoral nail for the fixation of an intertrochanteric fracture. Through the review of this case and literature, we would like to discuss the appropriate method for preventing this vascular complication and provide a method for early detection and treatment of a femoral artery injury occurring during the operation process mentioned above.
CASE REPORT
A 79-year-old male patient visited our hospital due to right hip pain and motion disturbance after a fall. According to the radiographic images, he had an intertrochanteric fracture without comminuted fracture fragments. The patient's medical history showed that he had been previously diagnosed with a right brain infarction and vascular dementia. However, he did not show noticeable neurological symptoms and was not taking any antithrombotic agents. The patient had also received a femoral nailing procedure due to a left intertrochanteric fracture three years ago. He was able to walk after the operation without any complication.
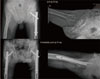
Four days after the injury, the patient underwent a closed reduction on a fracture table under C-arm image intensifier control before the operational management. For the closed reduction, we pulled the injured right limb as internally rotating 15°. After confirming proper fracture reduction, we further adducted the limb 20° for insertion of a femoral nail. After the closed reduction, we applied the following surgical procedure to the patient. First, a transverse skin incision was made from the greater trochanter tip proximally for 5 cm and the fascia of the gluteus maximus and the abductor muscle was subsequently split in line with its fibers. After insertion of a guide pin into the tip of the greater trochanter, a proximal femoral nail (Zimmer® Natural Nail™ System-Cephalomedullary Femoral Nail-Asia short; Zimmer, Warsaw, IN, USA), with a neck shaft angle of 130° was implanted over the guide pin. We used a lag screw (10.5 mm diameter and 90.0 mm length) and a distal interlocking screw (5.0 mm diameter and 27.5 mm length). During the surgery, satisfactory reduction and fixation were achieved without any representing complication (Fig. 1). The drainage tube was not applied because there was no sign of bleeding from the operation site.
One day after the surgery, the patient complained of pain and swelling on the injured thigh. On the second day, hemoglobin levels (Hb) dropped from 9.6 to 7.7 g/dL without any noticeable signs of bleeding. We transfused packed red blood cell (2 packs) to the patient. On the third day after the surgery, the patient experienced a temporary drop in blood pressure followed by rapid recovery. The general condition of the patient was stable. Therefore, we decided to monitor the symptoms further without medical intervention. However, the pain and diffuse swelling on the middle thigh were not alleviated and the Hb level dropped to 8.3 g/dL on the 7th day following surgery. The patient was subjected to computed tomography (CT) angiography of the lower limb. Using the CT, we identified a pseudoaneurysm adjacent to the perforating artery branch at the level of the distal interlocking screw, potentially due to blood vessel damage and intramuscular hematoma of anterior thigh muscle (Fig. 2). In response to this finding, a radiologist performed an angiogram and observed that the psedoaneurysm originated from the perforating branch of the deep femoral artery. He applied coil embolization with four micro coils to the damaged vessel under fluoroscopic angiogram control. After the coil embolization, radiographs confirmed the absence of an aneurysmal sac and further blood leakage (Fig. 3). On the 7th day following the embolization, the patient's thigh swelling remained and he was subjected to another CT angiography. The pseudoaneurysm was not visible, but a large hematoma in the rectus femoris was observed (Fig. 4). Additional aspiration using ultrasound guide was attempted but was not successful. We decided to monitor the patient closely. Fortunately, the patient did not present pain and swelling any longer. The patient started training with a walker and discharged 4 weeks after the initial operation.
DISCUSSION
It has been known that arterial damage occurring during the treatment of intertrochanteric femoral fractures is very rare; a review of the literature supports this. In 1964, Dameron1) reported a case with a deep femoral artery psudoaneurysm following the treatment of an intertrochanteric fracture2); after, additional cases were continuously reported. Major reasons for these arterial damages include 1) direct injuries due to fracture fragments3), 2) damages due to over-penetration of a drill bit, 3) prolonged irritation on a blood vessel wall owing to the protruding screws, and 4) injuries caused by improperly positioned retractors24). In addition, these types of injuries could occur throughout the various stages of the fracture episode including 1) direct damage by less trochanter fracture fragment when the injury is given3), 2) the surgical reduction process, 3) screw insertion, and 4) longstanding irritation of the inserted screw in the months and years following surgery5). The diagnoses of these psudoaneurysms can be made at different points as well. It has been frequently reported that diagnoses of the psudoaneurysms may be delayed from several hours to several months after the surgery6).
According to previous case reports, psudoaneurysms of the deep femoral artery were mainly found when dynamic hip screws were utilized4567). Recently, however, femoral arterial damages were reported throughout the literature related to surgeries using proximal femoral nailing for the treatment of the intertrochanteric fracture. Yang et al.8) and Grimaldi et al.9) reported superficial femoral arterial ruptures following the insertion of distal interlocking screws with Asian-Pacific type Gamma nail and Gamma 3 nail respectively. To our knowledge, however, there has been no case report to address the formation of a psudoaneurysm caused by the rupture of the deep femoral artery when proximal femoral nailing was used. These findings imply that the formation of a psudoaneurysm can occur both in superficial and deep femoral artery regardless of the fixation devices used. When the proximal femoral nailing procedure is used, the possibility of an injury to the blood vessel could increase because it is usually performed following adduction and internal rotation of the injured limb to make the insertion of nails easier. Furthermore in the process of reduction, a perineal post is used to draw the lower limb in. This could lead to the displacement of medial soft tissues towards the lateral side, place blood vessels closer to the femur and elevate the likelihood of arterial damages. Yang et al.10) conducted a study to observe changes in the superficial femoral artery with the color-flow duplex scanning. They found that the distance between the femur and the superficial femoral artery is significantly reduced when the patient's femur was in adduction and adduction-internal rotation positions compared to the neutral position. They also found that in 60% of cases, the distance was less than 10 mm when the lower limb was in the adduction-internal rotation position. In 8% of cases, the distance was even less than 5 mm. Given the results of this study, the authors recommend that interlocking screws should be inserted when a patient's femur is located in the neutral position.
Han et al.11) investigated the relationship between the insertion sites of interlocking screws and femoral arteries with CT angiography. Through their study, the authors addressed that 1) superficial femoral arteries are located anterior while deep femoral arteries are posterior and 2) average distances to the femur are 9.24-9.87 mm and 27.27-27.81 mm for deep femoral and superficial femoral arteries, respectively. This result implies that deep femoral arteries are more likely to be damaged during surgical procedures. The lag screw of a proximal femoral nail, used in the current case, has 15° anteversion to the main body. So, the distal interlocking screw is relatively inserted and located posterior. This feature could increase the risk of rupture of the deep femoral arteries.
Many cases have reported delayed diagnosis of these vascular complications. In the present case, we confirmed the diagnosis 7 days after the surgery, mainly due to the lack of recognition regarding this complication. Chong et al.12) suggested that there is a triad of symptoms for psudoaneurysm resulting from deep femoral arterial damages: 1) thigh swelling, 2) continuous bleeding of the fasciotomy wound, and 3) anemia with falling Hb levels. In our case, we did not notice bleeding on the surgical sites or subcutaneous hemorrhage. Rather, the patient experienced middle thigh swelling with pain, unexplained anemia and an episode of drop in blood pressure. Therefore, it is recommended that careful examinations should be performed when considering the possibility of blood vessel damage as suggested above.
In order to make an accurate diagnosis, non-invasive CT angiography could be a more appropriate choice rather than the ultrasonic Doppler. Ultrasonic Doppler may be limited in providing clear images of deep femoral arterial damages due to the location of the arteries. If the psudoaneurysm is confirmed by CT angiography, coil embolization would be the best alternative for treatment as demonstrated in the current case46). It is also possible to consider insertion of a stent-graft38) depending upon conditions of adjacent blood vessels. Recently, injection of thrombin has been used for treatment13). In some cases, surgical procedures would be options, including ligation of the psudoaneurysm through the surgical exploration to confirm arterial damages or direct removal of damaged blood vessels. Previous studies57), however, have addressed complications of these surgical methods, including postoperative infections and vast blood loss during surgery. Therefore, surgical treatment should be minimized.
To prevent the formation of a psudoaneurysm, it is advisable to release the traction and place the patient in the neutral position when inserting distal interlocking screws. Further, careful use of the drill bit is warranted. Excessive power should not be used when drilling to penetrate the medial cortical bone. Appropriate drill guides might be needed to avoid over-penetration of the femur.
In order to diagnose this type of vascular complication early, it is important to be aware and monitor signs and symptoms related to the possibility of postoperative blood vessel damage throughout intertrochanteric fracture surgical procedures. Specifically, it is highly recommended to consider the possibility of a psudoaneurysm when a patient presents with diffuse swelling and pain on the thigh in which surgery has been done, and unexplained anemia following the surgery. We recommend a diagnosis via CT angiography and coil embolization with angiography as the best option for the treatment of a psudoaneurysm after surgery for femur fracture fixation.



 XML Download
XML Download