

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Nowadays, following development of bearing system of hip arthroplasty, various combinations of metal, polyethylene and ceramic articulation are using as an alternative bearing. Each bearing system has their pros and cons, so not only metal on polyethlene (MoP) bearing but also ceramic on ceramic (CoC) or ceramic on polyethelene (CoP) are used in worldwide.
THR used CoC components showed excellent clinical result on short to mid-term follow-up, especially overall survivorship and other complications such as prosthesis failure, aseptic loosening and prosthetic joint infection12). However, ceramic fracture is still unsolved problem. Following development of ceramic bearing, the number of ceramic fracture was rapidly decreased but still there was reported 0.004% ceramic fracture on third generation ceramics and 0.002% ceramic fracture was reported on fourth generation ceramic articulation3). It remained one of the most catastrophic complication in CoC THR and we need revision THR surgery in all cases of ceramic fracture.
With the increasing the number of hip arthroplasty cases, the number of revision surgery also increasing. There is no definite consensus on the bearing choice of revision THR following ceramic fracture, but when we performed revision surgery using MoP articulation, we should alert cobalt intoxication caused by cobalt-chrome wearing. Until now some cases have been reported about cobalt intoxication including toxic heart failure in Western45). However, despite high incidence of CoC bearing THR in Korea, there was no previous report of cobalt intoxication after MoP revision THR following previous ceramic fracture. It is provisionally important issue but hard to diagnose at a glance. The objective of this case report is to present a fatal massive cobalt intoxication with heart failure induced by prosthesis wear and to inform that once we considering it, we could treat successfully this issue.
CASE REPORT
Fifty-three year old male presented to emergency room in our hospital with progressive shortness of breath. Symptom was started about 6 months ago so he visited local hospital. He worked up for worsening dyspnea. Simple chest radiograph and enhanced heart magnetic resonance imaging study were performed and they showed bilateral pericardial and pleural effusion. There was no evidence of ischemic change. Transthoracic echocardiogram showed the evidence of heart failure, left ventricular ejection fraction (EF) was 40%. A month later follow-up echocardiogram was performed and EF was checked below 31%, heart function getting worse. He was admitted at local hospital and started on vasopressors but urine output was decreased and follow-up echocardiogram showed a 25% of EF. Patient recommended heart transplantation and transferred our hospital emergency room.
In January 2002 and March 2005, he underwent sequential bilateral total hip arthroplasties due to alcohol-induced osteonecrosis of the femoral head using CoP bearing surfaces (C2 stem [Lima Corporate, Udine, Italy], 28-mm forte ceramic head [BIOLOX®; CeramTec Inc., Plochingen, Germany], cross-linked polyethylene liner and 54-mm SPH acetabular cup [Lima Corporate]). At 12 years postoperatively, he presented to the other hospital with acute onset of left hip pain. He was diagnosed ceramic head fracture on his left hip. Head and liner change revision surgery was performed using cobalt-chrome alloy 28-mm metal head and protruded cross-linked polyethylene liners by Lima Corporate. Following the operation record, the ceramic particles were located inside the joint capsule at revision surgery. Also at that time, his heart function was normal (EF=65%).
In our hospital, the patient admitted cardiovascular department in internal medicine. As the cause of heart failure, the medical team initially suspected autoimmune disease such as systematic lupus erythematosus. However, laboratory findings were not suspected. Patient complained nonspecific fatigue and general weakness but had no other symptoms such as visual and hearing loss, cognitive dysfuction. During work-up, patient presented progressive left hip pain and complaint of discomfort for the mass on the left groin. He also complained left leg weakness and numbness. Simple radiograph (Fig. 1) and enhanced computed tomography study (Fig. 2) was done. Simple radiograph image shows radiodense area around the hip joint and radiologist suspected heterotopic ossification. The cardiovascular department consulted orthopedic department. In the image findings showed huge mass combined hemorrhagic component lining acetabular component extending psoas compartment and eccentric wear on cobalt-chrome alloy metal head. Also highly radiodense material was seen around neck inferior portion and severly deformed metal head was seen. It was highly suspected that metal related granuloma, which means severe metallosis. Performed heavy metals screen, cobalt levels were 397,800 µg/L (normal range, 0 to 3.9 µg/L) and chrome levels were 236,000 µg/L (normal range, 0 to 3.0 µg/L) suggesting cobalt toxicity. Hip joint aspiration was done for decompression as radiologic intervention and ethylenediamine tetraacetate chelation therapy started immediately. After 10 cycle chelating therapy, metal level was lowered cobalt levels by 255.2 µg/L and chrome levels by 39.5 µg/L. Patient experienced symptomatic improvement and he was tolerable to tapering vasopressor. When hospital day after 134, medical condition of patient was getting improved, we underwent revision surgery.
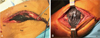
Following previous operation scar, posterolateral approach was done. Black and thick fluid gushed out immediately following incision tensor fascia lata (Fig. 3). Continually we exposed metal head by using trochanter osteotomy and could find severely deformed metal head. Not only eccentric wear on metal head, but defect of metal head was seen on apex of head. Trunnion was seen through the defect (Fig. 4). Meticulous removal all the visible ceramic fragments and aggressive debridement of involved soft tissue was done. We found the ceramic particle near lessor trochanter (Fig. 5), but complete remove all of the involved soft tissue was impossible. Removed all implants except the stem and repeated washings out of the joint space, CoC re-revision THR was done (Fig. 6) using option head. After the revision surgery, the patient’s general condition was more improved but remained left leg neuropathy. Nerve conduction velocity test and electromyography test was done and it suggested left femoral neuropathy. The patient discharged postoperative 79 days. Final heavy metals screen results were 27.79 µg/L on cobalt and 22.17 µg/L on chrome.
DISCUSSION
CoC bearing not only demonstrated the lowest wear rate in several studies but also highly resist scratch and biologically enert6). However the risk of breakage remains a major concern. Especially in Korea, comparing to western countries, most of surgeons favor CoC bearing surface up to 80%7), so ceramic fracture is more issued and ceramic fracture predicted to increase in near future. Also in present case, cobalt toxicity was diagnosed after MoP bearing revision THR following ceramic breakage. In western, there were some previous cases89) reported heart intoxication which used ceramic bearing as index surgery. However, most of them were manifestation combined other systemic complication such as auditory complication, hypothyroidism or neuropathy, but our case shows only heart problem and in our knowledge this is first report in Korea of toxic heart failure due to cobalt after THR.
Sometimes toxic heart failure due to cobalt intoxication after THR surgery is very hard to diagnose if we don’t have experience or if we are not considering about THR bearing choice. Especially the clinical manifestation shows only about heart failure like this case, usually internal medicine doctor contacts the patient first so it can be easily misdiagnosed or neglected hip problem. Also in current case, medical team suspect rheumatoid disease at first. Until diagnose cobalt toxicity cardiomyopathy it takes about two months after admission and we could do revision surgery about four months hospital day. Because the trends of bearing surface usage in THR in Korea are different from those in other Western countries, we should more consider about this issues following ceramic fracture and need toxicology work up when treat the heart failure patient who had history of arthroplasty. Also if we found abnormal toxicology result, we should consider not only chelation therapy but revision surgery as possible.
There are no definite consensus of bearing choice yet when revision THR following ceramic breakage which index surgery performed by CoC. The most popular bearing in revision THR after ceramic fracture is CoC bearing again and theoretically also ideal, but only a few clinical result and there were no long term study yet. Even there were also reported good clinical result of revision surgery using MoP bearing10), and some surgeons reluctant to use CoC articulation because concern about re-fracture of ceramic. But take into account like this devastating complications after cobalt-chrome wear caused by remained ceramic particles, we should carefully select which bearing is more safe.





 XML Download
XML Download