

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Idiopathic chondrolysis of the hip is characterized by extensive loss of articular cartilage, progression of joint pain, and a decreased range of motion (ROM) in the joint as the disease progresses. Because its etiology is not clearly established, a diagnosis should be made after ruling out infection, inflammation, trauma, and avascular necrosis of the hip joint that may also be causes of chondrolysis. Unfortunately, its prevalence rate is not well known, but the disease is known to be very rare and mainly occurs in adolescents. When an adolescent is diagnosed with the disease, conservative treatments, including pain control, traction and physical therapy, and using crutches to reduce weight bearing are all preferred; however, methods and timing of surgical treatment are still controversial1). Because the authors had experienced this extremely rare case of bilateral idiopathic chondrolysis of the hips in an adult male, we report this case through a review.
CASE REPORT
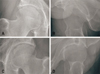
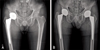
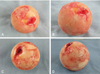
A 54 year-old Korean man visited the orthopedic surgery department due to persistent pain in his right hip joint starting a month previously and a gait disturbance was caused by this pain. He received a stent due to coronary artery occlusive disease in 2006 and received arthroscopic surgery for a rotator cuff tear in 2012. He did not have any notable medical history related to his joints, such as septic arthritis, tuberculosis, and rheumatoid arthritis. He was not undergone joint injection before. The pain started without any trauma about a month prior and worsened with exercises and walking. On a physical examination, he showed severe limping, no signs of rebound tenderness, and a positive sign to a Patrick’s test including a severe decrease in joint ROM (flexion, 100°; extension, 0°; abduction, 30° internal rotation, −5°, external rotation, 20°). Spine and sacroiliac joints did not show any significant findings upon physical examination. A simple radiograph showed no remarkable findings thus an magnetic resonance imaging (MRI) was conducted. Exudation in the right hip joint was increased, and his acetabular articular cartilage and acetabular labrum were almost completely obscured (Fig. 1A, B; Fig. 2A). His C-reactive protein and erythrocyte sedimentation rate were in the normal range. Serum markers for rheumatoid arthritis, including the rheumatoid factor, were also normal. The patient did not have a family history of rheumatoid arthritis. The patient was initially diagnosed with transient synovitis of the hip and arthrocentesis was administered after hospitalization. The findings of the hip joint fluid were all normal. After hospitalization, he was enrolled in a conservative treatment, including traction and physical therapy, yet he did not noticeably improve. Accordingly, a total hip replacement arthroplasty was performed one week later (Fig. 3A). The findings in the operating room revealed extensive chondrolysis of the articular cartilage in the head of the femur (Fig. 4A, B). From the biopsy, nothing other than the synovial vitreous body was found. Polymorphonuclear cells were not found (Fig. 5).
The patient did not experience any pain on the operated hip joint and revisited the hospital due to pain in his left hip joint one year after the surgery. The pain occurred without any trauma as in the first incidence. Similar to his previous visit, he severely limped, and again, displayed no signs of rebound tenderness, a positive sign to the Patrick’s test and a severe decrease in the joint ROM (flexion, 90°; extension, 20°; abduction, 30°; adduction, 10°; internal rotation, 0°; external rotation, 20°). Significant neurological findings in the lower body were not found. There were no remarkable findings on the simple radiography so again, an MRI was ordered. The MRI revealed an increased amount of joint effusion as noted in his left hip joint with much debris and bone marrow edema at the left acetabular roof and at the lateral portion of the femoral head, revealing cartilage thinning at the left acetabulum. Progressed degeneration of left labrum was compared to the prior MRI (Fig. 1C, D; Fig. 2B). We suspected chondrolysis of the left femoral head as was the same with the right side and thus the patient received a left-side, total hip replacement (Fig. 3B). Extensive chondrolysis of the right femoral head was uncovered during the surgery (Fig. 4C, D). The HHS (Harrison hip score) was 67 points preoperatively, which improved to a 96 points at the last follow-up. The VAS (visual analogue scale) score was 7 points preoperatively, there was not any pain at the last follow up. No complication was found during follow period. Currently, at 21 months after the right hip joint surgery and 9 months after the left hip joint surgery, the patient is not complaining of any symptoms and continues to enjoy his daily life.
DISCUSSION
Chondrolysis of the hip is characterized by extensive loss of hip joint cartilage and patients usually visit hospitals complaining of pain in the hip or knee joints. Chondrolysis of the hip was first reported in 1930 by Waldenström2), and various reasons including a slipped capital femoral epiphysis (SCFE), trauma, septic arthritis, rheumatic arthritis, and Stickler syndrome have all since been elucidated1). In 1971, Jones3) reported nine cases of patients who suffered from chondrolysis of the hip without any clear etiology. One report noted that the chondrolysis was not related to any SCFE, immobility, trauma, infection, and rheumatoid arthritis and they named this idiopathic chondrolysis of the hip. In 1975, Duncan et al.4) had suggested the following diagnostic criteria: 1, occurrence during adolescence; 2, gradual pain and limping; 3, progressive limitation in the ROM in the hip joint; 4, stricture of the articular cavity and line conservation of the femoral head in a simple radiograph; 5, aspecific synovitis; 6, unknown etiology.
Idiopathic chondrolysis of the hip in adults is less prevalent than that in adolescence. In 1995, Wada et al.5) in Japan reported two cases of patients who were 29 and 37 years old and Sivanantham and Kutty6) reported a case of a 20-year-old Native American in 1977. These cases also showed progressive hip joint pain and limitations of ROM without specific causes. In simple radiographs, the articular cavity had narrowed and the femoral head appeared normal. The results of the biopsies showed avascular necrosis, inner hyperplasia of the arterioles in the articular capsule, and nonspecific inflammatory findings in the articular capsule and synovial tissue. Bilateral idiopathic chondrolysis of the hip was reported by Rachinsky et al.7) in 2000, in which the patient was a 14 year-old teenager.
The patient we reported herein was a rare case of bilateral chondrolysis of the hips in an adult male. The patient complained of hip joint pain, walking disturbances, and limitations in his ROM. in simple radiographies, the articular cavities had narrowed and the femoral head was found to be normal. In this case, the patient did not have any underlying diseases that would have caused chondrolysis of the hip, so he received a biopsy during the surgery to determine a differential diagnosis. The histological findings of idiopathic chondrolysis of the hip are a thinning of articular cartilage, fibrosis, hypertrophic degeneration of cartilage cells, thickened articular capsule due to proliferation of the synovial membrane, and osteonecrosis. The biopsy results in this case were unremarkable except for the synovial vitreous body. The patient was not an adolescent, yet idiopathic chondrolysis of the hip was diagnosed due to the presence of extensive cartilage loss confirmed by naked eye and through radiographs.
Thus far, there have been no established diagnostic criteria for chondrolysis. A clinical diagnosis is made by excluding the etiologies that would cause acute or chronic hip joint pain1). The clinical presentations are characterized by rapid and extensive chondrolysis and show various stages of the disease entities from a complete recovery to fibrous ankylosing4). Simple radiography should be administered in the anterior-posterior and in the lateral planes of the hip joint to compare with the contralateral side but are to not be related to clinical symptoms and recovery. Protrusio acetabuli is an important finding that is worthy of notice especially in children who complain of unilateral hip joint pain8). MRIs can be useful because they can identify the changes of bone marrow faster than other imaging modalities. Bone scans and scintigraphy are highly sensitive. The Tc bone scintigraphy reveals an increase in uptake in the bilateral femoral head. The patient who has a gradual loss of their hip joint cavity and protrusion acetabuli at the same time should be suspected of developing idiopathic chondrolysis of the hip. All biochemical and microbial examinations revealed normal findings. These examinations include inflammation levels, joint fluid culture, and a rheumatic antibody examination. Generally, trauma can cause idiopathic chondrolysis of the hip so it is important to exclude trauma during any diagnosis. It should be noted that apparent hip joint fractures or dislocations can destruct the articular cartilage. Mankin9) reported the reaction of articular cartilage to mechanical trauma. He reported that subchondral lesions may remain on the articular surface like a scar and thus damaging joint congruency which in turn can cause secondary osteoarthritis.
To this day, etiology for intracerebral hemorrhage has not fully been explained. Thus, treatments have targeted symptoms only. Treatments are nonsteroidal anti-inflammatory drug or steroidal anti-inflammatory drugs, bed rest and skin traction to reduce workload on the hip joint, and use of crutches when walking. Physical therapy is important to maintain joint ROM during the first several months. Hip joint fixation must be avoided because it may cause joint stiffness and fibrous ankylosis. Surgical methods are still controversial; amputations of muscle and tendon, capsulotomy, and capsulectomy were conducted and have yielded various results4). For patients under 20 years old, a total hip arthroplasty may be effective in controlling pain but it has been reported that it also might cause durability problems, and thus should be a careful weighed option10). In this study, the patient was relatively old for the other surgical treatment options, we chose the total hip arthroplasty as a primary treatment option. However, we think that more case studies is needed to select optimal treatment of idiopathic chondrolysis of the hip in adult.
In conclusion, we report our treatment experience of bilateral idiopathic chondrolysis of the hip in an adult patient that was caused without any underlying diseases.


 XML Download
XML Download