

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Acetabular fractures are uncommon injuries with a rising trend in the developing countries. This could be due to increase in motor vehicle accident12). Increase in motor vehicle accident could be due to ignorance of traffic police and poor traffic system, all contribute to the incidence of this dilemma3). At present there are only few studies that address this particular issue. Acetabular fractures are challenging and complex injuries. These injuries require trained and expert orthopedic surgeons who unfortunately are less available in developing country like Pakistan34) as surgeons expertise and approach to particular acetabular fracture also influence the outcome56). Surgeons expertise required are fellowship trained surgeon and extensive pelvic and acetabular surgery experience. Acetabular fractures are major clinical problems as being the foremost weight bearing joint of the body. Lack of advances in radiological assessment and surgeon experience leads to conservative and delayed management of these fractures. This in turn results into various long term complications. Letournel7) proposed that surgical treatment of acetabular fractures has got better prognosis than conservative management in patients with acetabular fractures. Only a few setups in the country have the ability to manage these types of fractures. This study aims to evaluate the functional and radiological outcomes of surgical management of acetabular fractures among patients in tertiary care hospital.
MATERIALS AND METHODS
Total of 60 patients of either gender presented with acetabular fractures were enrolled. This was a prospective study conducted at the Department of Orthopaedic Surgery in Liaquat National Hospital (Karachi, Pakistan), a tertiary care hospital. The study was approved by the Ethics review Committee of hospital (0292-2016).
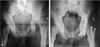
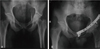
Patients who encountered between January 2012 and January 2014 were entered. Factors examined include age, gender, mechanism of injury, associated injury, time between injury and surgery (in days), preoperative degree of displacement, fracture pattern and quality of reduction. All the surgeries were performed by a single surgeon who is fellowship trained and had 15 year experience in pelvis and acetabulum surgeries. All patients had definite indications of surgery with more than 2 mm displaced acetabular fractures, articular impaction, unstable and non-concentric reduction, Matta roof arc angle less than 45°. The selection technique was case series study. Only those patients who had completed at least 24 months of follow-up were included in the study. Fractures were classified according to the Letournel-Judet classification system8). Out of 60 patients, 10 patients were lost to follow-up and were not included in the study. The remaining patients attended our outpatient clinic and was evaluated clinically with Harris hip score (HHS) and radiologically with Matta outcome grading910). To evaluate functional outcome patients were categorized into excellent (HHS, 90-100), good (HHS, 80-90), fair (HHS, 70-80), and poor (HHS, <70). These patients were further subcategorized into acceptable or not acceptable group. Patients with excellent to good outcomes are in acceptable group and fair to poor outcomes are in not acceptable group. All the patients underwent routine pre-operation assessment which includes thorough history (mechanism of injury), examination (overlying skin, neurovascular status) and imaging such as X-ray pelvis (anteroposterior view) and Judet views (iliac oblique and obturator views) to assess degree of displacement and fracture pattern. To evaluate the effect of degree of displacement on postoperative radiological and functional outcome, patients were divided into two groups (>2 mm displacement, ≤2 mm displacement) Preoperative radiographic evaluation shows fracture displacement of >2 mm in 15 cases and ≤2 mm in 35 cases. Fracture types were divided into simple and associated fractures which are then further classified into five subcategories as shown in Table 1. Surgeries were performed using various approaches and decision was mainly based upon fracture pattern and surgeon preference as well. Kocher-Langenbeck (n=25, 50.0%) approach was the most common surgical approach followed by ilioinguinal (n=16, 320%) and triradiate (n=9, 18.0%) approach. Open reduction and internal fixation of fractures were performed using reconstruction plates of 3.5 mm, screws (3.5 or 4.5 mm) or combination of plate and screws. Postoperative anteroposterior view of pelvis and Judet views (iliac oblique and obturator views) were used to assess the quality of reduction. The patients were categorized into three groups based on Matta radiological grading such as anatomical, congruent or incongruent. Anatomical if all fracture gaps and steps had been removed intraoperatively and postoperative films shows restoration of all five anatomical lines (ilioinguinal, iliopectineal, dome, posterior wall and anterior wall) with the head centered and parallel beneath the acetabular roof (Fig. 1, 2, 3). A congruent reduction was best judged on anteroposterior film which was useful in assessing the hip with reference to contralateral normal hip joint. Patients with poor restoration of five anatomical lines with inward subluxation of hip were included in the incongruent group (Fig. 4). Among these 50 patients, two patients (4.0%) had already been treated with total hip replacement because of developing secondary osteoarthritis between one and two years after open reduction and internal fixation of acetabulum. These patients were included in poor functional and incongruent radiological outcome.
The patients were followed up clinically and radiologically at six weeks, three months, six months, one year and two years. Patient's demographics and postoperative outcomes were noted in a predesigned study proforma and the data was analyzed using statistical package for social sciences (SPSS) version 20.0 (IBM Co., Armonk, NY, USA).
RESULTS
1. Baseline Characteristics
Out of 60 patients, there were 38 male and 22 female patients. Ten patients were lost to follow up and were not included in the study. Therefore there were 50 patients with complete data. The overall mean age of study subjects was 44.20±11.65 years. The mean duration of stay was 9.28±2.36 days. Mean time taken between injury and surgery was 5.00±3.59 days. The most common mechanism of injury was Motor vehicle accident 37 (74.0%) while in associated injury most common was extremities injury 24 (48.0%). Most of the patients 37 (74.0%) were admitted in ward rather than intensive care unit (ICU). Kocher-langenbeck approach was done in 25 (50.0%) patients. Regarding the presenting patterns of fractures, it was observed that simple fractures were seen in 42 patients while associated fractures seen in 8 patients. Traumatic sciatic nerve injury was found in 6 (12.0%) of patients. Four of the six patients had neuropraxia pre-surgery and had recovery with complete nerve function while no recovery of nerve function in two cases, both these cases had neglected injuries. Nerve conduction studies were performed at six weeks and at six months. During this period patients were managed conservatively in ankle foot orthosis splint. Tendon transfer was performed in two cases after a year. Infection detected in 4 (8.0%) while AVN femoral head was found in 2 (4.0%) of patients. Baseline characteristics are shown in Table 2.
2. Functional and Radiological Results
Functional outcomes were assessed using the HHS. Functional outcomes were divided into two group's; i.e., acceptable and not acceptable. On the basis of this division, 35 (70.0%) outcomes were acceptable and 15 (30.0%) outcomes were not acceptable. Stratification with respect to age, gender, mechanism of injury, associated injury, fracture pattern, time taken between injury and surgery and initial degree of displacement on radiographs was done to observe effect of these modifiers on functional outcome. The results showed that there was significant association of functional outcome with respect to age, mechanism of injury, time between injury and surgery and initial displacement on radiographs as shown in Table 3.
Radiological results were assessed using Matta outcome grading. Here the patients are divided into three groups such as anatomical, congruent and incongruent group. On the basis of this division, 39 (78.0%) outcomes are in anatomical group, 5 (10.0%) are in congruent group and 6 (12.0%) are in incongruent group. Stratification with respect to age, gender, mechanism of injury, associated injury, fracture pattern, time between injury and surgery and displacement on radiographs was done to observe effect of these modifiers on radiological outcome. The results showed that there is significant association of age, mechanism of injury, associated injury, fracture pattern, time between injury and surgery and initial displacement on radiological outcome as shown in Table 4.
DISCUSSION
Fractures of the Acetabulum though being un-common are of great clinical importance as being the most important weight bearing joint of the lower extremity. These fractures are mainly caused by high velocity motor vehicle accidents due to rise in incidence of motor vehicle accident. The incidence of these fractures is rising in developing countries in contrast to the United States and Western Europe where the incidence is stable11). These fractures need well-planned management treatment guidelines and expertise. In countries like Pakistan where adequate facilities are scarce and lack of well trained experts in the field, majority of the fractures tend to get managed conservatively. This leads to complications such as deep vein thrombosis, joint stiffness, hypostatic pneumonia12).
Our setup is one of the only few which have the capacity to deal with these types of fractures in the region. Mean time duration between injury and surgery in our study being 5.00±3.59 days is comparatively lower than study done from the neighboring country showing the mean injury surgery duration of 21 days13). Male gender being more common could be attributed due to the reason that males in this society are more involved in travelling purposes for various reasons14). Extremities injuries are more common injuries in these types of fractures15). Our study also shows that patients having any associated injuries most commonly in the extremities. Posterior wall fractures are the most common encountered fractures seen in our setup. This finding is consistent with international studies16). Sciatic nerve injury can be caused by acetabular fractures and the surgical interventions associated with fracture management. All the patients who presented to our setup had traumatic nerve injuries and none of the patients had iatrogenic injuries. In a study done by Lehman et al.17), the incidence of nerve injuries was found to be 4% on admission whereas in our study it was found to be 12%. This could be due to the reason that our study is limited to 50 cases and hence the true incidence of these nerve injuries might not be correctly calculated in countries like Pakistan where majority of patients do not come to hospital17).
The radiological outcome correlate significantly with the functional outcome and quality of reduction of fracture was the single most important predictor of clinical function, radiological grade and development of arthritis. Functional outcomes of the patients were measured using the HHS. In our case, mean HHS was found to be 82.36±8.55. This is slightly higher but still comparable to a findings mentioned by Shrestha et al.11) of mean HHS of 78; and 74 is a study done by Gupta et al12).
Postoperative surgical site infections are uncommon. Our study reports surgical site infection as 8.0%. In a study done by Suzuki et al.18), the surgical site infection was 5.2% superficial and deep infections combined, which is less than our study. In our study, all the patients had superficial surgical site infections with culture being positive for drug sensitive Staphylococcus aureus. These were treated with antibiotics and repeated dressings and the infections were recovered.
Following patients for up to 24 months, two (4.0%) patients developed osteoarthritis and subsequently underwent total hip arthroplasty. Both of these patients were elderly with mean age of 55 years and had initial displacement of >2 mm on initial radiographs. Our study reported that initial displacement of >2 mm had significant effect on both functional and radiological outcome. Meena et al.19) also demonstrates poor results with initial displacement of >2 mm. This shows that initial displacement of >2 mm is one of the prognostic factor for the development of osteoarthritis. Literature shows conversion of open reduction and internal fixation (ORIF) to Total hip arthroplasty in 28% of the patients among elderly population with mean age of 60 years. This is because of increased fragility of bones of elderly patients. In our study, the elderly study population comprised of 10%; five of the patient population and three of these patients had conversion of ORIF to arthroplasty among elderly which is 40% among elderly being higher than the findings of study done by O'Toole et al20).
Previous study concludes that delay in surgical reconstruction of acetabular fractures has worse effect on outcome2122). We evaluate the effect of delay in surgical reconstruction on outcome by dividing patients into two groups. Patients who were operated within a week had significantly better results than patients operated after one week. Letournel7) in his study concludes that outcome is worse if acetabular reconstruction were undertaken beyond three weeks.
Fracture pattern had significant effect on radiological outcome but not on functional outcome in our study. Kreder et al.23) found that functional outcome was significantly worse in patients with radiological arthritis and in those with associated posterior wall and posterior column fractures. We use the Letournel and Judet system to classify acetabular fractures that doesn't consider fracture comminution and displacement. This classification can guide surgeons about surgical approach but can't useful to assess functional outcome.
Associated injuries had no significant effect on functional outcome in this study. Moed et al.22) concludes that associated injury have significant negative effect on functional outcome.
CONCLUSION
Study results indicated that mechanism of injury, time between injury and surgery, initial degree of displacement and quality of reduction had significant effect on functional as well as radiological outcome. With the availability of good imaging facilities, surgeon experience, better instrumentation along with good perioperative care, we believe that the surgical fixation of displaced acetabular fractures would yield better results.






 XML Download
XML Download