

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Various directions of stress transmitted to the bone depending on muscle contraction, which occurs during the most of physical activities as it used. Continuous exposing to these repetitive stresses makes bone vulnerable to localized deformation or stress fractures of the bone. These stress fractures can occur often in frequent physical activity occupations, especially soldiers or athletes.
Although numerous factors, such as physiologic, mechanical, pharmacologic and systemic factors and so on can complexly affect to bone mechanostat responses, we still cannot assess which factor is more important than others on occurring stress fractures1).
Many studies and case reports reveal the mechanism and risk factors of stress fracture. However, there is no report, which explains the late diagnosed avulsion stress fracture at ischial tuberosity after short period of strict running motion yet. This report provides a case of stress fracture which occurred after 5 days of exercise which including hyper-flexion of the hip for each running motion.
CASE REPORT
A 19-year-old man presented to the orthopedic surgery department with pain in the left buttock after military training which including running with hyper-flexion of hip for 3 hours, twice a day for 5 days. When he hyper-flexed his left hip joint, he felt and heard a crack. Initially about one week later, he referred to the local hospital because of persisting hip pain. On radiographic evaluation, he diagnosed as pelvic bone fracture and recommended for further evaluation. However, he refused to get more examination due to the alleviation of the hip pain. Although he got rest without any military training for the next six weeks, there was no improvement and tingling sense developed over the posterior aspect of left thigh. During the first consultation with the patient, he complained difficulty on sustained standing and sitting on a locked position.
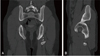
His body weight, height, hip and lumbar T-score for dual-energy x-ray absorptiometry (DXA) scan were 76 kg, 183 cm, –0.7 and –0.1 respectively. On physical examinations, there was no limitation on range of motion of the left hip joint. Also he could walk without any pain except mild tenderness on the area distal from the ischial tuberosity. On the radiographs of the pelvis anteroposterior and frog leg view (Fig. 1), there was a 35×40×20 mm sized bony fragment, 15 mm distance from the left ischial tuberosity. After the patient admitted to our hospital, he had an examination of computed tomography (Fig. 2) and magnetic resonance imaging for rule out pathologic conditions. There was a bony fragment at left ischial tuberosity, which was mainly from conjoined origin of biceps femoris and semitendinosus tendons without any bone marrow edema (Fig. 3). Overall, he diagnosed as old avulsion fracture at ischial tuberosity. He determined to get conservative treatment on condition of a gradual alleviation of the symptom. During the admitted 2 months, he just got rest and high intensity laser therapy. Thanks to the improvement except discomfort on running, he discharged and returned to his military unit.
DISCUSSION
Stress fracture can divided into two types, depending on the relations between bone and muscle. One is fatigue fracture, which generated by excessive muscular stress applied to the bone of normal strength. The other is insufficiency fracture that occurred when normal muscular stress is applied to weakened bone. It is important to distinguish one from another for understanding the patient's medical status. These stress fractures are well known to occur in soldiers and athletes2).
It is hard to distinguish avulsion fracture of ischial tuberosity from hamstring muscle strain since its symptoms and injury mechanism are similar. However, accurate diagnosis is significant as treatments are different respectively3). Many authors suggest displacement of 2 to 3 cm, painful nonunion, exostosis formation, neurologic symptom as an indication for surgery. While others report that some patients who had displacement of more than 5 cm eventually regained muscle strength nearly equal to contralateral leg4). Also, there is no definitive classification system or operative indication exists for avulsion fractures of the hip and pelvis yet. Therefore, more studies are needed to provide the reasonable treatment to patients.
The hamstring muscle complex consists of three biarticular structures (semitendinosus, semimembranosus, long head of biceps femoris) and one uniarticular structure (short head of biceps femoris). Though, there are several studies and different results that estimating the power of the hamstring muscle, commonly all the reports represented that the biomechanical load on biarticular hamstring muscles are the greatest during terminal swing phase of sprinting and the semimembranosus muscle generates the largest peak musculotendon force5). For instance, in a study, the peak musculotendon forces which stress to the ischial tuberosity as tensile force during stance and late swing was 13.09 and 19.22 N·kg–1 in average respectively6).
The ischial tuberosity serves as the origin for the hamstring muscle. Then the ischial tuberosity avulsion fracture can occur when suddenly flex the hip forcefully. However, the pelvis stress fracture accounts for less than 1% of all stress fractures1). Despite, the prevalence of hip pain, it can be difficult to find the exact underlying causes. Initial pelvis radiographs will be normal in up to 70% of patients with pelvis stress fracture1). So, the careful history taking, including medical history, strength and duration of activities and others should be done to prevent the misdiagnosis.
Basically, the stress fractures occur from overuse mechanism. The muscle contraction provokes the compressive, tensile and rotational stress to bone. Then the muscle contraction results in micro damage to bone. In this way, repetitive stress to the bone followed by crack and the accumulation of which results in the stress fracture7). There are numerous studies about risk factors of the stress fracture. Though various biologic, mechanical and many other predisposing factors can increase the patient's risk for stress fracture, crucial modifiable risk factors are participation condition of the bone, frequency, duration and intensity of the causative activity.
According to literature, stress fractures can occur well after the marathon of nearly five weeks8). It can also occurs in experienced runner if the training period or intensity rapidly rises. In this case, the patient got pain, 3 months after the date when he join to the military service. Then there was no military training or excessive running during the enlisted period. In addition, he did little exercise before enlisting to military. His T-score for DXA scan was almost normal. Furthermore, the strength of the bone estimated to have no problem regarding the patient had no specific underlying disease or fracture history. This case has its singularity that avulsion fracture has occurred during the 5 days of hip hyper-flexion running motion.
Notable point of this case is, unlike others normally do, this patient transmitted stress to hip using excessive hamstring stretching during the hyper-flexion, which is the extension of terminal swing phase, while in extension he gave avulsion stress to ischial tuberosity by hamstring muscle contracture. This proves running that include hyper-flexion running motion exerts excessive stress to ischial tuberosity which can be accompanied by fracture in short term.


 XML Download
XML Download