

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Stress fractures in children are commonly reported in the tibia, fibula, femur and metatarsals, and femoral neck stress fractures are rare1). Femoral neck stress fractures occur mainly in athletes, military trainees, physically hyperactive people, and patients with metabolic disorders or who are undernourished2). Since Devas3) first described cases of femoral neck stress fractures in children and classified the fractures into two types in 1963, only about 20 cases have been reported134).
Femoral neck stress fractures are easy to be misdiagnosed as a hip joint sprain or synovitis in children because of their rareness in skeletally immature children and the nondescript features in the early stage.
CASE REPORT
A 10-year-old boy, 147 cm tall and 40 kg weight, presented to our hospital with complaint of sustained bilateral hip pain for 4 weeks. The pain was getting worse while walking and spread throughout thigh. He showed positive sign of Patrick's test in bilateral hip and a slight limping gait and limited range of motion (ROM) on a physical examinations. The pain was relieved with rest and not occurred during night time. No history of trauma or underlying disease was reported. He practiced taekwondo as a hobby. Blood test results revealed no abnormalities, such as systemic disease or evidence of pyogenic coxitis.
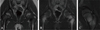
Radiographs showed a sclerotic line along the left femoral neck and evidence of callus formation. A minute disruption of the medial cortex at the trochanteric area was detected on the right side (Fig. 1). A magnetic resonance imaging (MRI) was taken to help with the diagnosis, and T1-weighted images showed decreased signal intensity along the left femoral neck and on the medial cortex of the right femur. T2-weighted images showed high signal intensity in the same area (Fig. 2).
The patient underwent conservative treatment with wheelchair ambulation and bed rest for 2 weeks. After 2 weeks, which was 6 weeks from the start of pain, he felt diminished bilateral hip pain and radiographs showed more sclerosis along the bilateral femoral neck, since then, partial weight-bearing ambulation with two crutches was permitted (Fig. 3A). Ten weeks from the start of pain, he did not complain of any discomfort and showed full ROM bilaterally. Radiographs indicated nearly complete bony union at the previous fracture site (Fig. 3B). Radiographs obtained 4 and 12 months after the initial pain developed showed complete healing of the stress fracture (Fig. 4).
DISCUSSION
Femoral neck stress fractures in children were first reported by Devas3) in 1963. He classified these fractures into two groups according to radiographs. The compression type, which account for most of stress fractures in children, typically show inferomedial cortical disruption initially, whereas a transverse type fracture, also known as tension type, tend to appear at the superolateral cortex5). Up to now, only one case of a bilateral femoral stress fracture has been reported in a child6).
The common symptoms of previously described cases were sustained hip pain and limping. Some cases had a history of excessive sports activity and problems affecting general health condition, such as anorexia nervosa27), whereas others had no clear contributory factors48). Our patient had no history of trauma or medical problems.
Radiographs are initially used to diagnose disease. However, in early stage of injury, it is difficult to detect a femoral neck stress fracture because of its nondescript features on radiographs. A few weeks after injury, it tend to appear as radiolucency through the cortex without any periosteal reaction. After two to eight weeks from the onset of symptoms, periosteal reaction or callus formation are generally seen as a result of bone remodeling9). However, MRI makes early diagnosis possible for patients who have clinical suspicion for stress fracture but radiographs are negative. Early resorption of bone can be manifested as local hyperemia and edema along the endosteal surface on MRI. Fat-suppressed T2-weighted images are important for detecting edema of the bone marrow. Several weeks after injury, a MRI shows bone marrow edema on both T1- and T2-weighted images and signal changes in the cortical bone. The common pattern of stress fracture on MRI is a low signal intensity line, surrounded by ill-defined large edema. The diagnosis of stress fracture was based on the presence of a focal, cortical and medullary zone of increased radionuclide uptake in all phases of bone scintigraphy. Although false-negative cases have been reported, bone scintigraphy has been considered as gold standard for early detection of stress fracture910).
The cortical interrupted region differs in compression (inferomedial) and tension types (superolateral) of femoral neck stress fractures. According to this classification, most fractures are the compression type and the remainder are tension type5). Given past experience, a compression type fracture usually does not require internal fixation and conservative treatment with limited weight-bearing is sufficient for healing6). However, an increased risk of displacement and a potential increase in osteonecrosis of the femoral head can occur in tension type fractures. Thus, patients with a tension type fracture must undergo internal fixation5). Differential diagnoses include hip joint strain, synovitis, osteoid osteoma, Legg-Calvé-Perthes disease, slipped capital femoral epiphysis, and malignant conditions such as osteosarcoma.
Because a femoral neck stress fracture is rare, it is easy to overlook in the differential diagnosis or may be misdiagnosed. Femoral neck stress fractures in children can be difficult to diagnose on plain radiographs. Thus, a femoral neck stress fracture should be considered in the differential diagnosis in children who present with sustained hip or groin pain, and MRI, close follow-up with serial radiographs should be performed.



 XML Download
XML Download