

 PDF
PDF ePub
ePub Citation
Citation Print
Print


The treatment of acetabular fractures is a complex area of orthopaedics that is being continually refined. Acetabular fractures generally are caused by high-energy trauma, and associated injuries are frequent. In patients with multiple trauma, medical contraindications from multisystem injury are common, even in previously healthy patients. And, complex fractures may require long operative procedures with significant blood loss. Furthermore, traditional surgical treatment requires extensive exposure, which may be complicated by infection, blood loss, wound healing problems, abductor weakness, sciatic nerve palsy, and heterotopic ossification12). Therefore, it seems reasonable to find less invasive surgical procedures to achieve the same goals as in conventional treatment. And, percutaneous screw fixation using two-dimensional fluoroscopy-based computerized navigation or arthroscopy may be more useful in multiple trauma patients3). In our study, we report two case of acetabular posterior wall fracture, which was treated through arthroscopic reduction and percutaneous screw fixation, with technical note.
CASE REPORT
1. Case 1
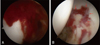
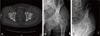
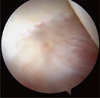
A 38-year-old man was injured in a car accident while driving, sustaining a left acetabular posterior wall fracture (Fig. 1). We explain to patient that it can be treated with non-weight bearing for 4 to 6 weeks, but he denied conservative treatment because he must return to his job. So, we decided to perform arthroscopic reduction and screw fixation after three days from trauma. Under spinal anesthesia, the patient was positioned supine on a fracture table with the affected limb in traction and the opposite limb. We made three portal (anterolateral, anterior, and posterolateral portals), the fracture fragment of the acetabular posterior wall was visualized after hematoma evacuation (Fig. 2). The fracture fragment was reduced into the intact acetabular side using a flexible guide wire through posterolateral portal. After anatomical reduction in the fracture site was confirmed by arthroscopy, we used a 4.0-mm-diameter cannulated screws to fixate the fragment under direct arthroscopic visualization (Fig. 3).
Postoperative radiographs and computed tomography (CT) was performed, the fragment was satisfactory reduced and compressed (Fig. 4). Within three days after the surgery, the patient discharged after care for postoperative wound and went back to normal life with crutch. After three months, we allowed to do light exercise like jogging. He did not complain pain or discomfort after six months from the surgery, began heavy sports activities. Since then he did not visit our clinic in over two years.
2. Case 2
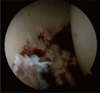
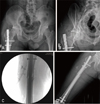
A 41-year-old man was injured in a car accident while driving, sustaining a right acetabular posterior wall fracture (Fig. 5A, B) and a right femur shaft fracture (Fig. 5C). Skeletal traction was initially attempted, we decided to perform closed reduction and intramedullary nail fixation for femur shaft fracture. In same time, we decide to perform arthroscopic reduction and internal fixation with screws for acetabular fracture, because of early rehabilitation. Under general anesthesia, femoral shaft fracture was treated by intramedullary nail system first. And, along the same way as Case 1, the fracture fragment of the acetabular posterior wall was visualized after hematoma evacuation (Fig. 6). The fracture fragment was reduced into the intact acetabular side using a flexible guide wire. After anatomical reduction in the fracture site was confirmed by arthroscopy, we used a 4.0-mm-diameter cannulated screws to fixate the fragment under direct arthroscopic visualization. After surgery, satisfactory reduction and compression were confirmed in postoperative radiographs and CT image (Fig. 7).
The patient was instructed to walk with partial weight-bearing with the aid of two crutches for four weeks after surgery. By three months post-operatively, he recovered full activities. After one year, femoral shaft fracture was united, we decided to removal intramedullary nail and to perform second look arthroscopy, we were able to confirm united acetabular fracture (Fig. 8).
3. Surgical technique
The patient was treated in the supine position on a commercially available hip arthroscopy distraction. We used a conventional anterolateral viewing portal and an anterior and posterolateral working portal and examined the joint space with a 70° arthroscope. After a blood clot and the bloody joint fluid had been aspirated, we examined the joint space and found the fracture site. We also found several osteochondral fragments in the cotyloid fossa. After capsulotomy was performed through the anterior to anterolateral site, joint debridement and loose body removal were perfomed. The fracture fragment was reduced into the intact acetabular side using a flexible guide wire. So, this technique is not available on severe comminuted fractures that are not compressed by screws.
At this time, must keep three notices in mind. First, check the size and shape of obturator foramen in intraoperative C-arm image are not different from preoperative obturator foramen view (Fig. 9). If size and shape are not same, tilt table like taking obturator foramen view. In this way, it will help to find accurate insertion site of a flexible guide wire.
Second, we need a curved guide because of curved acetabular shape. If you use straight guide wire, guide wire can penetrate articular surface. For this reason, we decided to use curved guide of Jugger Knot™ (1.4 and 1.5 mm, curved reusable guide; Biomet Inc., Warsaw, IN, USA) (Fig. 10). It can help to access easily to posterior wall of acetabulum, to maintain reduction by gently compressive force while a flexible guide wire was fixated.
Third, existing cannulated reamer is too short to access far cortex. So, you may make a choice among to produce long reamer, or to extend skin incision, in posterolateral portal, insert the shortest arthroscopic cannula deeply. After anatomical reduction in the fracture site was confirmed by arthroscopy, we used a 4.0-mm-diameter cannulated screws to fixate the fragment under direct arthroscopic visualization.
DISCUSSION
Acetabular posterior wall fractures can be treated with or without surgery. Nonoperative treatment generally consists of bed rest and traction followed by bed-to-chair transfer. Nonoperative treatment can be used in patients with simple, undisplaced, minimally displaced and those without free fragments in the joint.
The prolonged bed rest necessary for conservative treatment, however, can lead to different complications in elderly patients, including potentially life-threatening bed sores, pneumonia, and urinary infections. Elderly patients frequently have compromised strength, agility and balance, altered mental status, or neurological disorders. These patients are unlikely to comply with nonoperative management, and risk falling or involuntarily putting excessive weight on the injured limb, resulting in secondary fracture displacement4). Of course, surgery is not needed in simple acetabular fracture, but early internal fixation can help to avoid these complications in high-risk patients by simple and less-invasive surgery.
Arthroscopic techniques for fixation of intra-articular fractures offer the advantage of superior visualization and reduction of the articular surface, diagnosis and treatment5). It can also apply to acetabular fracture. Many author treated acetabular fracture with arthroscopic reduction and had a good result even in femoral head fracture and dislocation367). The additional benefits of this method were joint lavage and debridement of the hip joint. Joint debridement is known to be helpful in removing loose osteochondral fragments and might be helpful in reducing the risk of future osteoarthritis8).
Furthermore, arthroscopic reduction techniques offer another benefit for intraarticular lesions. In Case 2, patient had a metallic artifact, it would be impossible to obtain magnetic resonance imaging. So, this technique is a useful method for diagnosing and treating intraarticular lesions after hip trauma.
In Case 2, ipsilateral femoral shaft fracture was treated by intramedullary nail. So we worried about destruction of interlocking screw and distraction of fracture site by traction during hip arthroscopy. There is no reference about these problems, but Beutel et al.9) reported that in the patients with prior lower-extremity arthroplasty, the use of traction during hip arthroscopy is safe in this population. We applied gentle traction, fracture site and interlocking screw were visualized with fluoroscopy to confirm that traction was free of complications.
Although hip arthroscopy is technically more demanding, it is less invasive and can be easy way to return to normal life. However, there are concerns in relation to fluid extravasation creating compartment syndrome-type complications in the acute setting10). So, arthroscopic reduction technique will be good choice for acetabulum fracture, even in anterior or posterior column fracture, if only to overcome fluid extravasation. We observed closely intraoperative and postoperative monitoring of abdominal distention, core body temperature, and hemodynamic stability. High pump pressures may be risk factors, pump pressures were limited by 30-60 mmHg. And we tried to reduce operative time within 90 minutes.
Arthroscopic reduction and screw fixation technique is useful for reducing postoperative pain and achieving early return to activities for the patient. This technique will be tried in non-displaced and non-comminuted fractures, be the cornerstone to extend its indications with developments of techniques and equipments.





 XML Download
XML Download