

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Intertrochanteric and femoral neck fractures constitute the majority of hip fractures in the elderly. Early surgical intervention and ambulation are crucial to minimize complications123).
Femoral nail antirotation is commonly used to treat intertrochanteric fractures due to shorter operation time, less intraoperative blood loss, less limb shortening and shorter hospitalization in comparison with dynamic hip screw4567). Intramedullary nailing can be used to effectively control the sliding of the proximal fragment. Advantages of intramedullary nailing include biomechanical superiority and structural stability enabling immediate postoperative rehabilitation regardless of the fracture type456). Previous studies have reported favorable clinical and radiographic outcomes for proximal femoral nail antirotation (PFNA; Synthes, Oberdorf, Switzerland) with a helical blade and a single-screw-system (Gamma 3 Locking Nail System; Stryker, Schoenkirchen, Germany)8910).
Despite a number of intramedullary nailing advantages, 0-11.8% lag screw back-out has been reported1112). This is the most common reason for treatment failure, and may occur due to varus deformity of the femoral neck-shaft angle and superior cut-out of the lag screw. Baumgaertner et al.13) defined tip-apex distance (TAD) as the summation of the distance between the tip of the lag screw and the apex of the femoral head on the anteroposterior (AP) and lateral images. They showed that an increased TAD is a strong predictor of the lag screw cut-out14).
In the past, measurement of postoperative TAD was fulfilled using manual templates. Along with the rapid advancement in computer technology and digital imaging, picture archiving and communication systems (PACS) is widely used for transmitting radiographic images in the digital format15). Introduction of PACS has allowed easy access for adjusting screen brightness, measuring distances and angles and observing magnified regions of interest. These technological advances have shifted time-consuming manual measurements to simple and convenient measurements within a few clicks. It has enhanced the work efficiency in orthopedic surgery at several points including preoperative templating of the hip arthroplasty and measurement of postoperative TAD16).
It is difficult to take postoperative radiographic images in neutral position immediately after emergence due to pain. In addition, X-ray source to image distance and the location of the center of an image may vary in different clinical settings. Moreover, focus-film distance (FFD) is not consistently maintained due to different body contours. Therefore, we conducted this study to analyze the difference between measured and actual TAD values based on the degree of rotation and abduction using PACS.
MATERIALS AND METHODS
We used a femur replica (Synbone AG, Malans, Switzerland) with a femoral head diameter of 50 mm, a neck shaft angle of 135° and a femoral neck anteversion of 10. Similar to intramedullary nail insertion into the tip of the greater trochanter, PFNA nail and a helical blade were inserted into the replica (Fig. 1). The helical blade was 12.2 mm in diameter and 100 mm in length. The PFNA nail was 10 mm in diameter and 200 mm in length. The femur neck-shaft angle was 130°. The tip of the blade was placed at the inferior-center of the femoral head, the Cleveland zone 5 (Fig. 2)17). The TAD concept was first introduced for lag screw placement. In our study, the blade was located at a shallow-deep position to prevent cut-out of the nail18). AP radiographs were taken while the femur was held in neutral position and lateral radiographs were taken at 15° external rotation. FFD was consistently maintained at 1 m. The replica-film distance was also maintained at 1 m.
The replica-film distance was first fixed at 10 cm and radiographs were taken at neutral position and after applying 10°, 20°, 30° and 40° internal/external rotation to the mechanical axis. Subsequently, radiographs were also taken at replica-film distance of 20 cm under the same conditions. In the next step, radiographs were taken at replica-film distance of 10 cm and 20 cm after applying 10° abduction, and 10° and 40° adduction (Fig. 3). These conditions were based on different FFDs that clinically happen for the patient's radiographic positioning after reduction and internal fixation of an intertrochanteric fracture. We used PACS (Marosis; Maro Tech, Seoul, Korea) for analysis. PACS measures distances through magnification correction in radiographs. To acquire X-ray images with precise magnification, FFD was maintained at 100 cm and 100% magnification was applied to display the actual size. TAD values in neutral position were considered as standard values. An orthopedic surgeon and a radiologist, each measuring the TAD twice using PACS, measured the TAD in each image (Fig. 4). We used the mean value for analysis. The average error was 2 mm (4.5%) and the standard error was ±3.04. The maximum and minimum values were 55.77 and 37.35, respectively. Percent relative error was calculated using the following formula: Percent relative error=(experimental value-accepted value)/accepted value×100%.
RESULTS
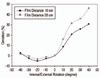
TAD values showed a percentage error of 3.9% after applying 10° external rotation at replica-film distance of 10 cm compared with the standard value. At 20°, 30° and 40° external rotation, percentage errors were 9.3%, 11.6% and 13.8%, respectively. TAD values showed a percentage error of 7.3%, 14.4%, 16.4% and 21.1%, respectively, after applying 10°, 20°, 30° and 40° external rotation at replica-film distance of 20 cm. The TAD showed an increasing tendency compared to the standard value when external rotation increased at both 10 cm and 20 cm replica-film distances.
In external rotation of the femur, a greater error was found at replica-film distance of 20 cm than 10 cm. In internal rotation of the femur, the TAD had a relative error of -1.3% compared to the standard value at replica-film distance of 10 cm. Errors were -2.3%, -1.1% and 1.2% after applying 20°, 30° and 40° internal rotation, respectively. Errors were -0.6%, -1.5%, -0.2% and 0.8% after applying 10°, 20°, 30° and 40° internal rotation, respectively, at replica-film distance of 20 cm (Table 1). In internal rotation of the femur, no significant tendency was observed with replica-film distance. Although the TAD decreased with an increase of internal rotation up to 20°, TAD values were close to standard value when the internal rotation angle was above 30° (Fig. 5).
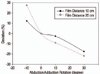
TAD values had a percentage error of 6.7% at replicafilm distance of 10 cm and 6.6% at 20 cm after applying 10° external rotation. In internal rotation of the femur, the TAD had a relative error of -1.4% and -9.6% compared to the standard value after applying 10° and 40° adduction, respectively, at replica-film distance of 10 cm, and a relative error of -1.5% and -9.8%, respectively, at 20 cm (Table 2). The TAD increased as the abduction angle increased and had a higher error at replica-film distance of 20 cm than 10 cm. Moreover, the TAD showed a decreasing tendency when the adduction angle increased, and a greater error was found at replica-film distance of 20 cm than 10 cm (Fig. 6).
In summary, TAD values increased consistently when rotation was applied from an internal rotation of 20° to an external rotation of 40°, while decreased with adduction compared to abduction. The TAD increased compared to the standard value when external rotation and abduction of the replica increased, while the TAD decreased when internal rotation (less than 30°) and adduction of the replica increased.
DISCUSSION
Baumgaertner et al.13) defined TAD as the summation of the distance from the tip of the lag screw to the apex of the femoral head on the AP and lateral images after magnification correction. Since then, a large number of studies have been performed to insert the lag screw into an appropriate location of the femoral head, and a TAD of less than 25 mm has been considered to reduce the risk of lag screw cut-out19). After Baumgaertner and Solberg14) proposed that an increased TAD is a strong predictor of lag screw cut-out, they verified that the use of the TAD concept improves the surgical outcome. Pervez et al.20) suggested that a TAD of less than 20 mm is ideal to lower the risk of lag screw cut-out.
We found that a significant error can occur in TAD measurement after internal rotation, external rotation, adduction and abduction of femur, and changes in replica-film distance. We found that TAD values were measured smaller than the actual size when the femur was adducted and internally rotated. TAD values were measured higher when the femur was abducted and externally rotated. Moreover, the TAD increased when replica-film distance increased during internal rotation and abduction. This is attributable to the tip of a helical blade being closer to the X-ray source in external rotation and abduction. Contrary observations with 30°-40° internal rotation could be the result of a change in the actual incidence angle of the helical blade tip. When the helical blade is not placed at the center of the femoral head, changes and errors in TAD measurement may occur.
Precise postoperative AP and lateral radiographs can lead to true TAD measurement. Deviation from the actual TAD with a consistent trend were seen on AP and lateral images based on the radiographic conditions. In addition, differences in TAD were observed with images taken under the same condition, which reflect the patient's size and replica-film distance increase.
Surgical management of intertrochanteric fracture is typically carried out on the fracture table. Internal/external rotation and adduction/abduction are applied for fracture reduction. In addition, it is difficult to take postoperative radiographs in the neutral position immediately after emergence due to pain. An error of above 10% was observed at an external rotation of above 30° in our study. For accurate TAD measurement, orthopedic surgeons should consider the external rotation of the femur when radiographs are taken in patients who tend to externally rotate their hips to reduce the pain.
The essence of our findings shows that surgeons need to be careful with many variables that may lead to errors in TAD measurement in the clinical settings. The actual TAD values are higher when the femur is adducted and internally rotated, and lower when the femur is abducted and externally rotated. Since the femur is internally rotated and adducted for reduction of most intertrochanteric fractures, the lag screw should be inserted closer to the apex of the femur because the actual TAD value is greater than what is measured on the C-arm image. Reflecting the patient's size, replica-film distance increases with obesity. Therefore, the actual TAD is typically smaller in patients with obesity. In obese patients, maintaining a consistently close distance between the C-arm source and the femur is proposed to be helpful in reducing errors in TAD measurement.
There are a number of limitations to our study. First, femoral neck-shaft angle (135°), femoral neck anteversion (10°) and location of the tip of a helical blade were inconsistent because the authors used a single femur replica. Hence, we were unable to identify changes and errors in TAD values according to changes in the femoral neck-shaft angle and placement of the tip of the helical blade. Second, the TAD showed a greater tendency to produce errors compared to our standard value (TAD=43.61 mm), since the blade was located at a shallow-deep position in the replica, while a favorable TAD is considered to be less than 25 mm in the clinical setting. Third, the average femoral neck-shaft angle is 125° and the average angle of femoral neck anteversion is 15° in Koreans21). The replica that was used in our study does not represent the femur in Koreans. Finally, there were no means for intraobserver and interobserver reproducibility.
CONCLUSION
The actual TAD values need to be considered more than the measured TAD when the femur is adducted and internally rotated, and less when the femur is abducted and externally rotated. In addition, the actual TAD values are assumed to be less in obese patients. For better evaluation of the TAD on intraoperative radiographs, orthopedic surgeons need to consider the insertion of the lag screw closer to the apex of the femur, because the femur is internally rotated and adducted for reduction. To accurately assess the TAD values after fixation of intertrochanteric fractures, AP and lateral radiographs should be taken in neutral position, and measurement error should be considered based on the patient's size.






 XML Download
XML Download