

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Compartment syndrome is characterized by an increase of compartment pressure induced by any number of causes including trauma, bleeding and compression, and can result in pain, motor and sensory impairment, ischemic tissue necrosis and other symptoms. The most common causes of compartment syndrome are fracture (about 69%) and soft tissue injury1), and the most common site is the lower leg, followed by the forearm2). This condition is frequently associated with tibial shaft fractures in adults, and its incidence rate ranges between 2.7-11%2).
This syndrome rarely occurs in the pelvic region and is more common in the lower legs and forearms. Since Petrick3) first described the initial case of gluteal compartment syndrome, it has been rarely reported. In fact, gluteal compartment syndrome without trauma, has only previously been presented in three domestic case reports456). In these three domestic cases, however, bleeding and hematoma occurred following the administration of anti-platelet agents or low-molecular-weight heparins. This paper reports a rare case of compartment syndrome of the gluteus medius occurring in the absence of trauma and with no hematoma or bleeding observed during surgery and includes a brief review of the literature.
CASE REPORT
A 50-year old man visited our hospital with a chief complaint of widespread pain in the right thigh and waist. He was undergoing outpatient treatment at the internal medicine clinic due to a history of diabetes, tuberculosis, and hepatitis C virus infection (Child-Pugh score class B). The patient was observed lying down in a supine position after taking 20 ibuprofen pills in an attempted suicide gradually entered into a stupor. The patient was admitted through the emergency room 8 hours after losing consciousness. After regaining consciousness, he complained of right thigh and back pain with a visual analogue scale (VAS) score of 8. Before loss of consciousness, he had no trauma and did not undertake any intense exercise.
The patient was 180 cm tall, weighed 95 kg and was obese with a BMI of 29.32 kg/m2. The pain described above was present at rest, but did not increase with passive flexion of the hip and knee. Compared to the healthy left side, swelling was detected in the right thigh, but no trauma was noted such as febrile sense or petechiae on the skin. Although circulation was normal in the right distal limb, diminished sensation was observed in the right thigh (80% of heathy side medially and 20% of heathy side laterally). At the emergency room, compartment pressures measured using Whitesides technique were 20 mmHg on the medial side and 40 mmHg on the lateral side (Fig. 1).
Laboratory findings included C-reactive protein 0.26 mg/dL (~0.5 mg/dL), lactate dehydrogenase 528 U/L (129-240 U/L), creatine phosphokinase 13,884 U/L (38-176 U/L), blood urea nitrogen 22 mg/dL (8-20) mg/dL, creatinine 1.32 mg/dL (0.6-1.2 mg/dL), and creatine kinase-MB 48.0 ng/mL (~0.5 ng/mL). All coagulation and bleeding parameters were normal with prothrombin time 14.0 sec (10.0-14.0 sec), international normalized ratio 1.28 (0.85-1.30), and activated partial thromboplastin time 40.3 sec (30-47 sec). A urine test revealed no ketone body, 3+ blood and 2+ protein. Although no deformed red blood cells were observed, both myoglobin and hemoglobin were detected in urine. Excluding swelling in the patient's hip and thigh (Fig. 2), no abnormal findings were observed on plain radiographs and computed tomography scans of the abdomen and lower leg at the time of admission. The patient underwent collaborative treatment with internal medicine after a diagnosis of liver cirrhosis and probable diagnosis of rhabdomyolysis, and sufficient amount of crystalloid fluid was given intravenously at the early stage. The initial compartment pressure measured using Whitesides technique was 40 mmHg on the right thigh. Although this was not a criterion for performing emergent fasciotomy, emergency surgery could be considered due to the severe pain and swelling of the thigh so a thorough follow-up was conducted. Until recovery to consciousness, the patient's position was not changed voluntarily or involuntarily. Pain (VAS 9) was intensified 8 hours after administration to the emergency room. The pain was localized to the right hip, and considerable pain was complained by the patient during passive range of motion exercises involving the hip. Diminished sensation below to 20% was noted over the calf and toes both medially and laterally. Flexor and extensor muscle strength on the ankle and toes was assessed as stage 1. Consequently, emergency fasciectomy and open release of the right hip were performed.
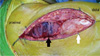
Open release was performed in a side-lying position. A 10-cm incision was made directly inferior to the greater trochanter and parallel to the posterior boarder of the greater trochanter at the height of the anterior superior iliac spine. The subcutaneous layer was dissected along the incision line, and a large volume of transudate was drained in this process. Compression caused by hematoma was not seen. Through an incision of the subcutaneous layer, the gluteus maximus fascia was exposed and then incised to the center of the greater trochanter. After the incision, decompression was achieved after a large volume of transudate was drained without any hematoma. There were no specific intraoperative findings in the vastus lateralis of the right thigh. Hematoma was not present in the three compartments of pelvic region (iliopsoas compartment, gluteus medius-minimus compartment, and gluteus maximus compartment)7), but severe swelling and ischemic change leading to a purple-black color were detected in the gluteus medius (Fig. 3). After fasciotomy, pain was improved and sensation was recovered in the affected legs by over 80% of the healthy side 48 hours after surgery. Muscle strength also improved to stage 3 or higher. On the third day post surgery, aseptic dressing and sufficient irrigation were performed in the operating room. Hip swelling gradually subsided and reperfusion was observed as the ischemia improved. On the fifth day post surgery, the incision site was sutured as ischemic changes were recovered (Fig. 4). Follow ups were continued for six months after surgery. Compartment syndrome was improved without loss of sensation and motor function and muscle weakness.
DISCUSSION
Compartment syndrome occurs when the tissue pressure within a muscle compartment exceeds the capillary perfusion pressure and results in decreased perfusion and ischemic changes. When the ischemic condition persists, the tissues and muscles undergo necrosis can lead to fibrosis in those muscle and tissues2). Trauma is the most common cause of compartment syndrome, and the calf is the most common area of onset1). Gluteal compartment syndrome is a rare condition that is caused by persistent compression of the hip subsequent to trauma, bleeding or hematoma, or is caused by remaining in the same position for a long period of time.
The diagnosis of acute compartment syndrome is typically made following clinical evaluation. In this case report, the first complaint of pain was delayed in the early phase because the patient was under a stupor due to drug overdose, and the location and boundary of the pain were unclear. After the patient regained consciousness, he complained of progressively intensifying pain. Aggravating pain and weakening sensation and motor function have been frequently associated with involuntary movement in patients with compartment syndrome8). Like in this review, as vague pain in the waist and thigh became definite pain in the hip over time, severe pain developed during involuntary movement of the hip. Before surgery, diminished sensation and muscle strength over the right leg is thought to be attributable to sciatic nerve compression caused by swelling and elevated compartment pressure in the hip and thigh regions.
Notably, the patient's first complaint was pain in the right thigh and leg and not hip pain. For this reason, compartment pressure was measured in the thigh only because thigh compartment syndrome was more suspected. Careful assessement of the gluteal compartments was not made. The pelvic region is divided into three compartments, the iliopsoas, gluteus medius and minimus, and gluteus maximus, and thigh muscles are divided into anterior, posterior and adductor compartments. For these reasons, all compartments need to be evaluated separately on physical examination9), but a complete exam was not performed in the initial phase. In the diagnosis and evaluation of compartment syndrome of the lower limbs, the possibility of gluteal compartment syndrome should be taken into account in patients complaining of thigh and back pain.
Gluteal compartment syndrome is a very rare condition10). In the present case, compartment syndrome occurred in the right gluteus medius among the gluteus compartments without any traumatic event or hematoma. This could be attributed to gluteal compression caused by remaining in a lying down position for prolonged periods of time after decreased consciousness due to drug overdose in obese state with a BMI of 29 kg/m2 or higher. Since the gluteus medius muscles are relatively small compared to the gluteus maximus and there is no space between the gluteus medius and maximus muscles, compartment syndrome of the gluteus medius seems to occur. This review supports past research recommending that gluteal compartment syndrome can develop from continuous compression of the hip by maintaining limited movement or improper posture for prolonged periods of time due to medication or trauma.
This review highlights that gluteal compartment syndrome can be caused by remaining in a side-lying position for a long period of time in overweight patients. Therefore, even though a patient initially complains of pain in the waist and thigh without any trauma, a thorough clinical evaluation of the gluteal compartments, in addition to the femoral region is warranted. If compartment syndrome is suspected, sufficient examination of all compartments associated with the pain can lead to more prompt diagnosis and adequate treatment including rare gluteal compartment syndrome.



 XML Download
XML Download