

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Although the exact pathological mechanisms of avascular necrosis of femoral head (AVNFH) are not fully understood, both non-traumatic (including excessive consumption of alcohol, corticosteroid overdose, Caisson disease, hemoglobin disorder(s) [e.g., sickle cell anemia], Gaucher disease, and radiation [e.g., chemoradiation therapy]123)) and traumatic causes (e.g., femoral neck fracture, dislocation of the hip) have been known to cause blood circulation disorders, thereby changing normal cellular physiology and eventually resulting in necrosis45).
Given the high efficacy of conservative treatment (s) for AVNFH, it is recommended that surgical interventions follow image diagnosis and/or when classified as necrosis with symptoms67). However, techniques aimed at preserving the femoral head, including core decompression, and vascularized/non-vascularized bone graft which are often advised for early necrosis, have shown varying clinical outcomes89101112). For these reasons, further investigations to better understand the effectiveness of these conservative treatments are warranted.
Following the accidental discovery of extracorporeal shock wave therapy's (ESWT's) osteogenic effects in animals in the mid-1980s, it was first applied to the treatment of musculoskeletal disorders13). Although the underlying mechanisms of ESWT are not fully understood, multiple studies have reported on its use for various cases and its effects on enhancing callus formation in delayed union14), re-vascularisation in overuse tendonopathy (e.g., plantar fasciitis and lateral epicondylitis of elbow joints)15), and tissue regeneration15).
Based on the impact of ESWT on vascularization and osteogenesis, a number of researchers employed it as a treatment for early stage AVNFH and reported improved clinical prognosis and decreases in osteonecrosis13). Further, there are a number of studies that compared clinical outcomes of ESWT to conservative drug treatments (e.g., the prostacycline-analogue iloprost16) and alendronate17)) and surgical treatments (e.g., core decompression, bone graft, and total hip arthroplasty), yet scant information is available regarding changes in clinical aspects and the effects across varying radiographic stages.
Therefore, in the present study, the authors: 1) divided enrolled subjects who were staged using Association Research Circulation Osseous (ARCO) into two groups; group 1 (stages I and II) and group 2 (stage III) and 2) carefully analyzed sequential clinical outcomes of ESWT to further investigate its effects in different radiographic stages. The overall significance of the study is to compare clinical outcomes of ESWT for varying radiographic stages of AVNFH.
MATERIALS AND METHODS
1. Study Subjects
Subjects who were: 1) diagnosed as AVNFH (≤ARCO stage III) from March 1993 through March 2012, 2) treated with ESWT, and 3) were able to follow-up at least two years, were included in this study. Based on these inclusion criteria, a total of 32 hip joint cases were analyzed retrospectively. The average age of subjects was 47.8 years and 12 subjects were classified as having idiopathic osteonecrosis (with no known risk factors). According to the analysis, eight and three subjects had history of alcohol consumption and steroid use, respectively. Traumatic necrosis (e.g., dislocation of hip joint) was identified in two members of group 1 and a single member of group 2 (Table 1).
2. Study Method
For this study, radiographic classification of osteonecrosis was made based on the ARCO staging parameters following evaluation of radiographs and magnetic resonance imaging (MRI). Failure was defined as 1) progression in radiographic stage or 2) the need for arthroplastic surgery before the two-years follow up as a result of clinical exacerbation. Postoperative clinical assessments were conducted using the visual analogue scale (VAS) score and Harris hip score (HHS)18). To compare the clinical assessments by degree of osteonecrosis (as classified per the radiographic stages), subjects were divided into two groups: i) the "early" osteonecrosis group (group 1, ARCO stages I and II) and ii) the "mid" osteonecrosis group (group 2, ARCO stage III). At the initiation of the study, 10 patients (13 cases), 6 patients (7 cases), and 8 patients (12 cases) were classified into the ARCO stage I, ARCO stage II, and ARCO III, respectively (Table 1). Comparisons between the two groups were conducted at 3, 6, 12, and 24 months after treatment. During patient visits, anterior, posterior, and lateral radiographs were taken to evaluate changes in lesion size, degree of expansion of cartilage degradation, and degenerative hips719). The mean follow-up period was 27 months.
3. Treatment Method (Fig. 1)
For all patients, the treatment was performed using the OssaTron orthotriptor (High Medical Technology, Kreuzlingen, Switzerland); ESWT procedures were performed under local anesthesia and in the absence of general anesthesia. With the guidance of the C-arm, the ESWT was focused on areas adjacent to femoral head necrosis. Prior to the procedure, lidocaine gel was applied to the skin and apparatus to minimize both the loss of energy of the extracorporeal shock and pain. As described previously, each patient received 6,000 shocks of extracorporeal shock (27 kV strength) per session4514). Next the groin areas were visually inspected for petechia, edema, and hematomas. Following treatment, patients were given no weight bearing restrictions and no additional drug or exercise treatments were provided.
4. Statistical Analysis
Median values of VAS and HHS scores were compared for all patients. Additionally, the Wilcoxon signed-rank test was performed to compare median VAS and HHS values between groups (as divided by the ARCO categorizations described above). SPSS ver. 16.0 (SPSS Inc., Chicago, IL, USA) was used and a P-value less than 0.05 was considered statistically significant.
RESULTS
The results of clinical assessments for both groups receiving ESWT are summarized in Tables 2 and 3, respectively. In the final follow-up assessment, there was a statistically significant improvement in the VAS score for both groups; the median VAS value increased by 1.5 points (P<0.001) and 4 points (P=0.056) in groups 1 and 2, respectively. Additionally, group 1 (i.e., those with "early" osteonecrosis) displayed a dramatic improvement (65.6 points vs. 95 points; P<0.001) yet such an effect was not demonstrated in group 2, those staged as ARCO III (47 points vs. 52 points; P=0.280; Table 3).
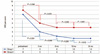
In addition, in subsequent follow-up observations, we saw significant improvements in the pain scores in both groups 3 months after therapy. However, such improvements were not demonstrated in subsequent follow-ups (i.e., 6, 12, and 24 months after therapy; Fig. 2). For HHS, group 1 showed significant improvements 3 and 6 months after treatment when compared to their pre-treatment levels (before therapy vs. 3 months after therapy, P<0.001; before therapy vs. 6 months after therapy, P=0.024) (Fig. 3).
In both groups, patients who received ESWT showed significant improvement in night pain; however no further improvement was noted in cases where there are serious limited joint angle ranges. According to radiographs taken at the final follow-up, one patient in group 1 improved from ARCO stage II to ARCO stage I. In addition, one patient in the ARCO stage I patient was also significantly improved. In group 2, one patient improved from ARCO stage III to ARCO stage II, also according to radiographic findings (Fig. 4). Important to note that there were two cases who underwent total hip arthroplasty after six months due to serious pain after the therapy. Lastly, there were no cases showing any complication on the site of treatment such as hematoma or sacral infection. One patient complained of numbness at the site of treatment, however, it was no longer a complaint at the final follow-up.
DISCUSSION
The major findings of the present study are that all patients with early and mid osteonecrosis (i.e., ARCO I and II stages) who underwent ESWT showed significant improvements in pain reduction and HHS. In contrast, such effects were not pronounced in the group 2. Lastly, in all cases, dramatic improvements in scores were seen three months after therapy.
ESWT is a type of sound wave with high pressure and velocity that can pass through liquid and soft tissues; when it goes toward bone, reflection and precipitation of the shock wave are made on the boundary surface between soft tissue and bone20). It has been suggested that these precipitations might positively impact necrosis and angiogenesis and multiple studies demonstrated its therapeutic potential on AVNFH13). Specifically, it was reported that ESWT may improve function of and pain around affected parts and reduce the severity of osteonecrosis2122). In line with these studies, the present work demonstrated that significant relief of pain was achieved by therapy over time. In group 1, our analyses indicate that significant improvement in HHS was achieved. In contrast, such improvements were not seen in cases where a patient had necrosis that had progressed enough to limit joint movements and function. In these cases, it was difficult to expect dramatic improvement in functions following therapy. Of note, however, most patients experienced clinical satisfaction due to the reduction of pain threshold including night pain.
ESWT has been widely utilized for chronic painful tendonopathy including lateral epicondylitis of elbow joints and plantar fasciitis15). Mechanisms responsible for pain in tendonopathy include abnormal delivery mechanisms, innervations of reduced vascular sympathetic nerve branches and increased secretion of non-vascular substance P by sensory nerves. This therapy induces angiogenesis of the affected parts, increases blood supply and recovery tissues thereby treating chronic inflammatory tissues and removing the abnormal symptoms associated with chronic pain1523). In fact, using an animal model, Wang et al.4) reported that the site of treatment with an extracorporeal shock wave overexpressed a variety of angiogenic factors including endothelial nitric oxide synthase, vascular endothelial growth factor, and proliferating cell nuclear antigen6) and promoted osteogenesis5242526). The promotion of angiogenesis has been known to facilitate blood supply for femoral heads thus contributing to bone remodeling and regeneration.
There are several non-invasive therapies for the treatment of AVNFH in addition to ESWT; in one report, Desai et al.22) show that alendronate may suppress osteoclasts to delay bone resorption hence preventing the early collapse of femoral heads. In another study, Levin et al.27) demonstrated that hyperbaric oxygen reduces the ranges of femoral head necrosis in rats. Furthermore, Disch et al.16) reported that iloprost, a prostacyclin analogue which has been used to treat Buerger's disease, might be also be an effective treatment for osteonecrosis. Of note, in agreement with results herein, Wang et al.4) showed favorable clinical outcomes of ESWT in conjunction with the alendronate treatment.
As shown in Figures 2 and 3, clinical outcomes assessed in the study were improved relatively quickly following therapy (3-6 months). In addition, although significant improvement in HHS was not demonstrated in group 2, pain scores were on the border of statistical significance. Additionally, except for one patient who progressed to ARCO stage III, no aggravating radiographic findings were demonstrated. There were two cases within group 2 who underwent total hip arthroplasty due to persistent pain and dysfunction after 6 months of the therapy, yet one of these cases showed radiographic improvement from ARCO stage III to II.
There are several limitations of the study; it was retrospectively conducted and is a single-arm study without control group. In the study, however, the authors regularly monitored clinical outcomes of ESWT in reference to the degree of necrosis and time. It is expected that results herein may provide important data for clinicians. Lastly, it is warranted to further confirm effects of the therapy on actual bone edema as well as osteonecrosis utilizing MRI in future.
CONCLUSION
ESWT improved the VAS pain score and HHS at 24 months follow-up for AVNFH patients, including those classified as ARCO stage I, II and III. In most cases, these clinical effects were pronounced within 3-6 months after therapy. Taken together, ESWT might be an effective alternative to achieve clinical improvements (e.g., pain and HHS) in this patient population prior to surgical intervention.






 XML Download
XML Download