

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Amongst unstable intertrochanteric femoral fractures, the type 3 fracture, defined by the Association for Osteosynthesis/Orthopaedic Trauma Association (AO/OTA) classification, is characterized by a reverse oblique fracture1), and its distal fracture fragments tend to be displaced inwardly due to a loss of inner cortical bone, resulting in extremely unstable fractures, both anatomically and dynamically, as compared to other intertrochanteric femoral fractures2). Recently, the results from a small number of studies have demonstrated favorable clinical outcomes for elderly osteophorosis patients with the type 2 intertrochanteric femoral fractures who underwent bipolar hemiarthroplasty (BHA)34). Additionally, a few studies have reported results from the use of open reduction and internal fixation using various fixing tools in type 3 intertrochanteric femoral fractures, which are expected to be very unstable256789). However, there have been no published reports comparing the clinical and medical imaging results between BHA and internal fixation. Therefore, the present study compared clinical results via a retrospective analysis of the implementation of either open reduction-internal fixation (OR-IF group) or BHA for treating type 3 intertrochanteric femoral fractures, as defined by AO/OTA classification, in elderly patients ≥70 years of age.
MATERIALS AND METHODS
Amongst a total of 982 surgical cases of intertrochanteric femoral fractures implemented between January 2005 through July 2012, 85 cases were type 3 reverse oblique intertrochanteric femoral fractures based on the AO/OTA classification. Of these, 18 cases were excluded for reasons including being <70 years of age, an inability to ambulate before their injury, and having one or more an accompanying or pathological fractures. Out of remaining 67 cases, the 53 cases with available follow-up data were analyzed retrospectively. The criteria for intertrochanteric femoral fractures included class 3 type fractures and cases representing free lateral wall fracture fragments owing to one or more additional lines on the coronal or sagittal planes of the femoral lateral wall. This study protocol was approved by the institutional board of Gwangju Veterans Hospital (GJVH-IRB No14-9-7).
Study patients were divided into either the OR-IF group (31 cases) or the BHA group (22 cases), and the reduction status was further divided into three groups for evaluation based on the classification system of Fogagnolo et al.10), which was slightly modified from that of Baumgaertner et al11). As results, 26 cases and two cases were classified as good and acceptable cases, respectively, while three cases were found to be poor. For internal fixation of the OR-IF group, the gamma locking nail (Trochanteric gamma locking nail; StrykerTrauma GmbH, Schonkirchen, Germany), proximal femoral nail (Synthes, Paoli, Switzerland), and proximal femoral nail antirotation (Synthes) were utilized for 11, 9, and 11 cases, respectively. A cementless, double tapering C2 femoral stem with a rectangular surface (Lima Corporate, Udine, Italy) was utilized for all cases in the BHA group.
The age of the total patient population ranged from between 70 and 86 years and averaged 77.6 years. There were 16 male and 37 female patients. The average follow-up period was 42.84 months (range, 24-68 months). In order to evaluate the level of patient hip functioning, the Harris hip score was used12), and the Singh index13) was used to assess the degree of osteoporosis. No statistical differences were noted between the study groups (i.e., OR-IF group and BHA group; Table 1). Forty seven patients (88.7%) had one or more accompanying diseases including hypertension, which was the most prevalent (28 cases), diabetes, cardiovascular diseases, cerebrovascular diseases, and pulmonary diseases.
All cases in which accompanying lateral wall fractures were found when visiting our hospital or type 1 or 2 intertrochanteric femoral fractures occurred during hospitalization, were divided in advance of the analysis depending on time of injury (i.e., time when the injury was sustained versus time before surgical implementation). Due to the inherent nature of the retrospective study design, it was impossible to describe clear criteria for the selection of operation methods. However, BHA was generally chosen for patients with one or more internal diseases, such as hypertension, cardiovascular diseases, diabetes, and renal diseases. Similarly, hemiarthroplasty was generally chosen for patients with expected early ambulation due to poor patient compliance, and for those in whom a high risk of internal fixation was anticipated due to the severity of the degree of pulverization of the femoral cortical bone. For both groups, anesthesia risk was assessed as well14) (Table 1).
1. Operation and Post-operative Treatment
On average, operations were implemented 3.5 days after the injury occurred. Of 53 cases, 50 (94.3%) underwent operations within one week (Table 2). Utilizing the fracture operation table and image amplifier, the closed reduction was performed for the OR-IF group until satisfactory reduction was achieved. Otherwise various surgical tools (e.g., clamp, and Hohmann retractor) were employed through a small incision around the fracture fragments for the reduction. No direct incision was made for the fracture site in any case. In cases where left reduction of fracture fragments was required, a thick Steinman pin was inserted to maintain the fracture prior to the introduction of the proximal femoral nail. The fixation of the lesser and greater trochanters during operations for those in the BHA group was performed only if a final femoral stem was inserted prior to assembly of the bipolar femoral head with the stem in order to complete the reduction of the joint and recovered the length of the leg. If a lesser trochanter was fractured, the displaced lesser trochanter was not separated from the iliopsoas tendon, but instead was placed manually on the anatomical positions prior to fixation via tying either the lower trochanter or upper/lower trochanter with a steel wire. In order to achieve stable fixation in cases involving a fractured and displaced lateral wall, the trochanters were properly placed on their anatomical positions prior to the use of a Dall-Miles cable or steel wire tied in the shape of an "8" for the lower part of the lesser trochanter and upper part of greater trochanter. If stable fixation was not achieved for the greater trochanter or lateral wall, additional holes were made for one or more femoral bones and the greater trochanter in order to allow for the steel wire to be tied in the shape of an "8" for further stable fixation. In cases where fixation was not achieved using a steel wire due to small fracture fragments or a serious degree of osteoporosis, the Ethibond suture was employed. Preventive medication for deep vein thrombosis or ectopic bone formation was not used, while compress dressing was provided after the surgery. Intravenous administration of antibiotics was given after five days from the surgery. Immediately after surgery, patients performed active bending and stretching exercises for their knee and ankle. One day after the surgery, patients started sitting on the bed. Wheelchair walking was allowed two days after the surgery, while ambulation was further allowed depending on the degree of pain, and bone union status, which was confirmed by medical imaging examinations, as well as reduction status.
2. Assessment Method
Patient data were analyzed retrospectively. More specifically, operation time, the amount of blood loss, and post operative compilations were compared between the groups. Further reoperation and operative methods were also analyzed. In order to compare short-term mortality, the difference in mortality within two years from the surgery was compared as well. Two independent orthopedic residents who did not perform any of the included surgeries performed clinical and medical imaging examinations and evaluations. Medical imaging evaluation included anterior, posterior, and lateral radiological images taken after surgeries, as well as more recent radiological images, which were compared and reviewed.
1) Evaluation of mortality
Because the present study included elderly patients ≥70 years of age, short-term mortality, defined as death within two years after the surgery, was analyzed. Regardless of the follow-up period, comparisons were based on the time of investigation, and patient information was obtained from the termination date of insurance from the National Health Insurance Corporation of Korea, as well as a reported date of death from a government office. Furthermore, actual death and time of death were confirmed retrospectively via medical histories from the hospital and phone interviews.
2) Clinical assessment
For both groups, operation time was recorded from anesthesia administration to the end of the surgery. Further, the amount of blood loss, blood transfusion, post-operative complications, and reoperation cases were assessed. In order to evaluate clinical parameters, these were monitored before/after surgery, and at the third, sixth, 12th, and 24th month follow-up periods. Functional evaluation was assessed using the Harris hip score12). Joint pain evaluation was assessed via the visual analog scale (VAS) scores (0=no pain, 100=unbearable pain)15).
3) Medical imaging assessment
Cases accompanied by a fracture of the lateral wall were analyzed in both groups. These cases were subdivided into those in which the fracture on the lateral wall occurred during the course of injury, those in which type 1 or 2 fractures according to the AO/OTA classification were diagnosed as a result of injury, and those in which a fracture was diagnosed as either type 1 or 2 when injured and went on to develop to type 3 due to a fracture on the lateral wall during hospitalization. As part of the medical imaging evaluation of the OF-IF group, bone union period was also monitored and defined as time taken for the formation of 3-4 cortical callus bridges according to anterior, posterior, and lateral radiological images taken after the surgery, as well as the absence of pricking and pressing pain when weight was loaded. Joint union was evaluated via dividing the reverse oblique intertrochanteric femoral fracture by the minor fracture line for the major fracture line. Moreover, other complications including secondary introversion via changes in the neck-shaft angle, degree of displacement of the distal fracture fragment, cracking of fixatives, perforation of the head of the femur, loosening of a screw or blade, and fracture non-union were investigated by comparing radiographic images taken immediately after the surgery and at the final follow-up.
For the medical imaging assessment of the BHA group, acetabular erosion, measurement length of both legs, and ectopic ossification according to the Brooker classification16) were monitored. Images were rated for the radiolucent line accompanied by a sclerotic line according to the method of Gruen et al17). Osteolysis, vertical offset, and stability of the femoral stem were measured at the final follow-up according to the method of Engh et al18). In addition, bone union of the lateral wall fracture, as well as time taken for its union, were recorded and compared. The vertical offset of the femoral stem was measured based on the method previously described by Callaghan et al19). To accomplish this, the distance between the center of a small hole in the proximal part of the femoral stem and the middle of the lesser trochanter was measured. The medical imaging assessments were performed by two orthopedic residents who were not involved in the surgeries. In order to validate the two methods of evaluation (between K1 and K2) the kappa coefficient test was performed. As a result, both evaluators were successfully validated for all measured parameters (K1=0.88, K2=0.81).
RESULTS
1. Mortality Assessment
Of all 67 cases, 14 had less than two years of follow-up. Among these 14 cases, 12 were excluded due to death. Five and seven of these subjects were from the OR-IF group and BHA groups, respectively (P=0.125). Of the 12 excluded cases, nine of the subjects died within one year of their surgeries. Four cases were from the OR-IF group and five were from the BHA group (P=0.268). Lastly, of the nine cases that died within one year of their surgeries, two (one from each group) died within three months (P=0.742).
2. Comparisons of Operative Blood loss and Operation Time
Regarding the amount of blood loss during the surgery, the BHA group lost 293.2 mL (range, 200-400 mL) while the OR-IF group lost 142.3 mL (range, 70-260 mL), which differed significantly between the groups (P=0.000). In contrast, there was no difference in operation time, defined as the time taken from the administration of anesthesia through the end of anesthesia, between the groups. In the BHA group, the average operation time was 67.0 minutes (range, 40-90 minutes), while it was 67.3 minutes (range, 40-90 minutes) in the OR-IF group. This comparison did not reach the level of statistical significance (P=0.960; Table 2).
3. Clinical Assessment
In the evaluation of early ambulation after the surgery, the average time taken for partial weight loaded walking with a walker or crutches was 9.3 days (range, 4-14 days) in the BHA group. In contrast, it was 13.6 days (range, 9-21 days) in the OR-IF group and therefore significantly shorter in the BHA group (P=0.032). It should be noted that although it took a shorter period of time, the hospitalization period was not significantly different between the groups (35.8 days [range, 24-58 days] and 40.4 days [range, 21-60 days] in the OR-IF group and BHA group, respectively; P=0.365). The Harris hip score was evaluated over four times beginning from three months after the surgery through the end of the follow-up period (i.e., 24 months after the surgery). According to the Harris hip score, there was no difference between the groups until the third measurement (e.g., third month [P=0.122] and 12th month [P=0.708] from the surgery), yet scores were significantly better in the OR-IF group when measured 24 months after the surgery (P=0.001). In contrast, the BHA group was found to have better VAS scores15) on the measurement performed three months after the surgery (P=0.043), while no differences were found on the sixth and 12th month measurements (P=0.546 and 0.436, respectively) from the surgery. In contrast, the OF-IF group had better outcomes as compared with those of the BHA group in the last assessment performed 24 months after the surgery (P=0.000; Table 3).
4. Medical Image Assessment
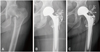
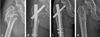
Of the 31 cases in the OR-IF group, 28 were accompanied by a fracture on the lateral wall. In contrast, 20 of 22 cases in the BHA group exhibited lateral wall fractures. In one case, a patient was diagnosed as type 2 intertrochanteric femoral fracture when hospitalized, but went on to develop type 3 reverse oblique fracture due to an additional fracture on the lateral wall while staying in our hospital (Fig. 1). In the OR-IF group, the most frequent position for a femoral head screw was Zone 5 (n=25 cases)20). After the first surgery, 26 of 28 cases in the OR-IF group and 16 of 20 cases in the BHA group displayed a minor fracture line union. The average time for this union was 9.2 months (range, 6-20 months) and 9.1 months (range, 4-15 months) in the BHA and OR-IF groups, respectively. No statistical differences in the union of the minor fracture line (P=0.089) or the average time taken for union (P=0.154) were detected between the groups. Of the 31 cases, in the OR-IF group, with the exception of one case involving artificial joint replacement due to early loss of reduction, one case of BHA due to of periprosthetic fracture, one case of additional surgery attributable to non-union, and one case of non-surgery treatment, 27 cases were able to achieve major fracture line union after their first surgery. The average time taken for the major union was 6.9 months (range, 4-13 months). Regarding the radiographic evaluation, neither radiolucent lines more than 2 mm suggestive of dissociation of the femoral stem nor vertical offsets of more than 5 mm were observed at the final follow-up. Furthermore, no osteolysis was detected. None of the subjects experienced a limb length discrepancy of >10 mm. Results pertaining to the stability of the femoral stem, assessed according to the method of Engh et al.18), demonstrated that 19 cases (86.3%) had bony fixation while three (13.6%) showed a fibrous stable fixation. No case showed ectopic ossification. Five and three cases from the BHA group and OR-IF groups, respectively, showed a displacement >5 mm during the union of the lateral wall; however, this difference did not reach the level of statistical significance (P=0.327; Table 4, Fig. 2).
5. Evaluation of Complications and Reoperation
Reoperation was performed for four cases. These cases were all from the OF-IF group. Of these cases, one required BHA due to periprosthetic fracture. The other cases included an operation for removal of an internal fixative, as the patient complained of severe discomfort (Fig. 3), as well as an autogenous bone graft and additional inner fixation using a metal plate and screws due to wide-spread bony defects and non-union. In the last case, BHA was performed due to early loss of reduction (within two months from the first operation). Of the two cases of non union of the major fracture line in the OR-IF group, one case was revised with bone grafting and additional plating, which achieved successful bone union. The other case remains under long-term follow-up and is monitored regularly, as no significant pain was noted and the patient declined to undergo reoperation in favor of using crutches (Table 5, Fig. 4). On the other hand, one subject in the BHA group complained vigorously about stimulation of the internal fixative. More specifically, the patient felt uncomfortable with the projected steel wire used for the fixation of the lateral wall. Even though the lateral wall was displaced upwards due to non union, conservative treatment is being provided, as additional surgical treatment is contraindicated due to the patient's current physical condition. This patient is currently able to walk with low walkers. In both groups, no cases of infection were detected.
DISCUSSION
Type 3 reverse intertrochanteric femoral fractures, as defined by the AO/OTA classification, account for 2% and 5% of total hip fractures and intertrochanteric femoral fractures, respectively5). This AO/OTA classification fracture type indicates a case where the fracture line extends to the distal part, toward the lateral femoral part, and over the left vastus ridge21). In such cases, the support afforded by the medially localized cortical bone is lost, resulting in a distal fracture fragment that tends to be displaced inwardly, making it very anatomically and mechanically unstable.2) It has been characterized as a four part burst fracture in elderly patients22). These burst fracture fragments can be classified into four types: a proximal fragment including the femur head; an anterior fragment including the trochanteric line; a posterior fragment including the trochanteric crest; and a distal fragment including the femoral shaft22). It has been reported that such cases require careful treatment, as the lateral wall is often fractured, and bone defects can be widely spread22). Anatomically, the lateral wall indicates the lateral femoral cortex from the vastus ridge to the distal part. Although it is a part of the lesser trochanter, the lateral wall also constitutes the most proximal extension of the femoral shaft and therefore serves as a lateral buttress in bone union. Because a high reoperation rate has been associated with cases involving one or more lateral wall fractures, accurate and rigid fixation has been considered an important factor for the determination of a prognosis of type 3 intertrochanteric femoral fracture accompanied by lateral wall fracture23). In a study conducted by Haidukewych et al.5), 49 cases of reverse oblique intertrochanteric femoral fractures were analyzed. All cases in the study had additional fracture lines that were non displaced and mostly extended toward the proximal greater trochanter. The study authors commented that surgeons should pay extra attention as a medullary cavity nail is inserted through the greater trochanter where the fracture line is extended, especially if a proximal femoral medullary nail is being used.
In the present study of elderly patients ≥70 years old, 48 had accompanying lateral wall fractures, indicating that it is not unusual to find this type of fracture, which most often occurs in elderly patients, in conjunction with type 3 intertrochanteric femoral fractures. As mentioned, we encountered one case in which a patient who was diagnosed as type 2 intertrochanteric femoral fracture advanced to type 3 due to an additional lateral wall fracture experienced during hospitalization in advance of the surgery. Therefore, the utmost care should be taken for patients with severe osteoporosis and a type 2 intertrochanteric femoral fracture characterized by a thin lateral wall. From the results of our previous studies, we determined that the minor fracture line, the lateral wall fracture, takes more time to achieve union as compared the major fracture line. This may be attributable, at least in part, to the force generated by the abductor muscles directed towards the lateral wall fragment. Additional investigations are warranted, as accurate assessment may be difficult to achieve based on such a small numbers of cases. In the treatment of reverse oblique intertrochanteric femoral fractures, sliding hip screws are not recommended due to surgical difficulty and lack of stable fixation, which elevates the reoperation rate 8-fold624). Therefore, it has been recently reported that intramedullary metal nails may be useful for such cases. The surgical treatment for type 3 intertrochanteric femoral fractures is characterized by short operative times, a small amount of blood loss, the inward displacement of the distal fragment, and complications78). Lower of delayed union may require reoperation for elderly osteoporosis patients, as well as for failure of internal fixatives9). Although we experienced difficulties in reduction due to burst reverse oblique fractures, the reduction was performed as closely as possible to the anatomical features in order to achieve rigid internal fixation, thereby resulting in favorable outcomes at the final follow-up. However, in the treatment of unstable reverse oblique fractures in osteoporosis patients, either implementation of reoperation for elderly patients who may already have comorbidities, or asking patients to stay in bed for long periods to avoid weight bearing due to the occurrence of complications (such as loss of reduction after internal fixation) may be somewhat risky and burdensome. In addition, results from recent reports have demonstrated that primary BHA allows patients to ambulate earlier with a low failure ratio34). Subsequently, this surgical approach (i.e., BHA) was studied in order to determine if it conferred favorable results in reverse oblique intertrochanteric femoral fractures. Although BHA allows for early ambulation and lowers the risks of reduction failure and complication occurrence associated with internal fixatives, its inherent surgical disadvantages (e.g., large surgical incision, large amount of blood loss, and long operative time), as well as other risks (e.g., dissociation of artificial joint, acetabular erosion, infection, and dislocation) have hindered its widespread application. BHA for intertrochanteric femoral fractures is expected to be associated with a larger amount of blood loss and longer operative times as compared to those of reduction and internal fixation, yet these findings were not supported by the data from the cases in the present study. Specifically, we did not find any difference in the surgical times between the OR-IF BHA groups. This may be attributable to the longer amounts of time required to prepare patients with fractures on a surgical table and to perform reduction, even though the actual amount of time taken between incision and suture was short.
BHA in reverse oblique intertrochanteric femoral fractures represents its own advantages, as there was no difference in operative time compared to internal fixation, early ambulation was achieved, patients rarely complained of early pain, and reoperation was not necessary. It should be noted that although not statistically different between groups, there were four cases of non union of the lateral wall in the OR-IF group (out of 20 cases) while only two of 28 cases were reported in the BHA group. These consequences may have been attributable to the subluxation of soft tissues attached to abductor muscles and lateral walls during the processes involved in the anterior-lateral approach method. Therefore, selection of the optimal approach method should be carefully determined in cases with intertrochanteric femoral fractures accompanied by lateral wall fracture treated via BHA. In addition, three of 22 cases experienced a limb length discrepancy, which represents a slightly higher frequent rate as compared to our previous experiences with BHA. This was likely the result of difficulties in achieving an accurate measurement of the greater trochanter tip due to the lateral wall fracture. Additionally, a complete reduction for the comminuted fracture of the lesser trochanter, which can be used as a reference for the estimation of limb lengths, was not made. Therefore, further efforts are required in order to produce more accurate measurements of limb lengths in BHA.
In cases where comminuted fractures of the greater trochanter are accompanied by reverse oblique inter trochanteric femoral fracture, anatomical reduction and rigid fixation of bone fragments are significant due to consequences including hip pain and changes in the lever arm covering the center of the hip throughout to the abductor muscle's point of action, potentially resulting in dislocation of an artificial joint due to weakened abductor muscles25). Various surgical techniques are being utilized for treating unstable intertrochanteric femoral fractures via BHA262728). In the present study, we utilized the tension band wiring technique which fixes the lesser trochanter with a circular steel wire. Subsequently, another steel wire was penetrated through the upper greater trochanter and the lesser trochanter in an "8" shape28). The advantages of the technique included its simplicity, its lack of effect on surgical costs, and the lack better bone union, bursitis, bone resorption, and damage to the metal plates employed for rigid fixation26). In particular, it reduces operation time, which may be crucial for faster recovery times in elderly patients. In contrast, we found five cases where displacement (<5 mm) was noted in the BHA group despite the use of a steel wire for fixation. Although the fractured lateral wall was fixed with the steel wire in an '8' shape, the displacements we noted may indicate how difficult it is to maintain closure owing to the action of the abductor muscles. It should be noted that in cases where the lateral wall has fracture in parallel with the ground, there is a greater likelihood of lateral wall fragment displacement, as stable wire fixation is difficult to achieve.
The present study had a few limitations. Firstly, we were not able to clearly define the criterion for the selection of the surgical approaches based on our retrospective study design. Second, the follow-up period (i.e., two years) was relatively short. Lastly, the number of cases was somewhat small due to the low incident rate of type 3 fractures. Therefore, future prospective studies with larger sample sizes and longer follow-up durations may be warranted. Considering its significance, further investigations regarding the various surgical techniques used to attach the greater trochanter, as well as matters that require attention during BHA surgery should be performed.
CONCLUSION
In the final follow-up of elderly patients (>70 years old) with reverse oblique intertrochanteric femoral fractures, favorable clinical outcomes associated with pain as well as functionality, were demonstrated. In conjunction, successful anatomical fracture reduction and rigid internal fixation were achieved. Therefore, stable internal fixation may be a good choice for healthy patients with excellent bone quality that can reasonably expect to live long lives. Appropriate reduction of fractures is available through careful examination of fracture types in advance of surgery. Due to its benefits (e.g., early ambulation, pain improvement, and low risk of reoperation), BHA may be chosen for cases with severe bone pulverization and poor bone quality, patients with a higher risk for early failure, as well as for those with short remaining lifetimes, and patients who require early ambulation, as high risks of complications are expected due to long term bed rest.







 XML Download
XML Download