

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
We evaluated the short term results after treatment of cam type femoroacetabular impingement (FAI) by arthroscopy.
Materials and Methods
We evaluated the clinical and radiological results of arthroscopically treated cam type FAI in patients who had failed conservative treatment with hip pain, with at least 12 months follow-up, from November 2010 to December 2012. There were 19 males and six females. Mean age of patients was 32.9 years (19-57 years) and mean follow up period was 17.2 months (13-31 months). We analyzed the alpha angle, head neck offset, visual analogue scale (VAS), and modified Harris hip score (MHHS).
Results
Mean alpha angle improved from 64.8° to 39.9° and mean head neck offset also improved from 0.8 to 7.6 mm. Peripheral longitudinal and radial fibrillated labral tear was the most common in the anterosuperior quadrant. Damage to acetabular cartilage was identified in 14 patients. Mean VAS improved from 6.3 to 0.9 and mean MHHS improved from 51.7 to 73.6. Complications associated with the operation included three cases of femoral head articular cartilage injury, two cases of pudendal nerve injury, and two cases of lateral femoral cutaneous nerve injury.
Figures and Tables
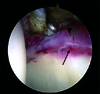 | Fig. 1Arthroscopic finding shows the labral contusion (arrow head) and peripheral longitudinal tear (arrow) at anterosuperior quadrant of the acetabulum.
|
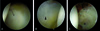 | Fig. 2Variable articular cartilage lesions. According to Outerbridge classification, (A) grade 2 partial thickness defect of cartilage (arrow); (B) grade 3 partial thickness defect with diameter more than 1.5 cm (arrow head); and (C) grade 4 full thickness acetabular cartilage defect (asterisk) can be seen.
|
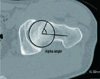
 | Fig. 3Pre-operative anteroposterior (A) and frog leg (B) radiographs of the left hip show asphericity of femoral head and mild pistol-grip deformity and negative head-neck offset and alpha-angle. Alpha angle is shown at B and D. Post-operative anteroposterior (C) and frog leg (D) radiographs show restored sphericity of the femoral head and restored impingement free head-neck offset. The head-neck offset is distance between two parallel lines (B, D).
|


References
1. Ganz R, Parvizi J, Beck M, Leunig M, Nötzli H, Siebenrock KA. Femoroacetabular impingement: a cause for osteoarthritis of the hip. Clin Orthop Relat Res. 2003; (417):112–120.
2. Tannast M, Goricki D, Beck M, Murphy SB, Siebenrock KA. Hip damage occurs at the zone of femoroacetabular impingement. Clin Orthop Relat Res. 2008; 466:273–280.

3. Ganz R, Leunig M, Leunig-Ganz K, Harris WH. The etiology of osteoarthritis of the hip: an integrated mechanical concept. Clin Orthop Relat Res. 2008; 466:264–272.
4. Siebenrock KA, Wahab KH, Werlen S, Kalhor M, Leunig M, Ganz R. Abnormal extension of the femoral head epiphysis as a cause of cam impingement. Clin Orthop Relat Res. 2004; (418):54–60.
5. Lavigne M, Parvizi J, Beck M, Siebenrock KA, Ganz R, Leunig M. Anterior femoroacetabular impingement: part I. Techniques of joint preserving surgery. Clin Orthop Relat Res. 2004; (418):61–66.
6. Beck M, Leunig M, Parvizi J, Boutier V, Wyss D, Ganz R. Anterior femoroacetabular impingement: part II. Midterm results of surgical treatment. Clin Orthop Relat Res. 2004; (418):67–73.
7. Beck M, Kalhor M, Leunig M, Ganz R. Hip morphology influences the pattern of damage to the acetabular cartilage: femoroacetabular impingement as a cause of early osteoarthritis of the hip. J Bone Joint Surg Br. 2005; 87:1012–1018.
8. Crawford JR, Villar RN. Current concepts in the management of femoroacetabular impingement. J Bone Joint Surg Br. 2005; 87:1459–1462.
9. Leunig M, Beaulé PE, Ganz R. The concept of femoroacetabular impingement: current status and future perspectives. Clin Orthop Relat Res. 2009; 467:616–622.
10. Ganz R, Gill TJ, Gautier E, Ganz K, Krügel N, Berlemann U. Surgical dislocation of the adult hip a technique with full access to the femoral head and acetabulum without the risk of avascular necrosis. J Bone Joint Surg Br. 2001; 83:1119–1124.
11. Byrd JW, Jones KS. Arthroscopic management of femoroacetabular impingement: minimum 2-year follow-up. Arthroscopy. 2011; 27:1379–1388.
12. Byrd JW, Jones KS. Arthroscopic femoroplasty in the management of cam-type femoroacetabular impingement. Clin Orthop Relat Res. 2009; 467:739–746.
13. Guanche CA, Bare AA. Arthroscopic treatment of femoroacetabular impingement. Arthroscopy. 2006; 22:95–106.
14. Larson CM, Giveans MR. Arthroscopic management of femoroacetabular impingement: early outcomes measures. Arthroscopy. 2008; 24:540–546.
15. Philippon MJ, Briggs KK, Yen YM, Kuppersmith DA. Outcomes following hip arthroscopy for femoroacetabular impingement with associated chondrolabral dysfunction: minimum two-year follow-up. J Bone Joint Surg Br. 2009; 91:16–23.
16. Clohisy JC, McClure JT. Treatment of anterior femoroacetabular impingement with combined hip arthroscopy and limited anterior decompression. Iowa Orthop J. 2005; 25:164–171.
17. Laude F, Sariali E, Nogier A. Femoroacetabular impingement treatment using arthroscopy and anterior approach. Clin Orthop Relat Res. 2009; 467:747–752.
18. Nötzli HP, Wyss TF, Stoecklin CH, Schmid MR, Treiber K, Hodler J. The contour of the femoral head-neck junction as a predictor for the risk of anterior impingement. J Bone Joint Surg Br. 2002; 84:556–560.
19. Tannast M, Siebenrock KA, Anderson SE. Femoroacetabular impingement: radiographic diagnosis-what the radiologist should know. AJR Am J Roentgenol. 2007; 188:1540–1552.
20. Goodman DA, Feighan JE, Smith AD, Latimer B, Buly RL, Cooperman DR. Subclinical slipped capital femoral epiphysis. Relationship to osteoarthrosis of the hip. J Bone Joint Surg Am. 1997; 79:1489–1497.
21. Stulberg SD, Cordell LD, Harris WH, Ramsey PL, MacEwen GD. Unrecognized childhood hip disease: a major cause of idiopathic osteoarthritis of the hip. In : Cordell LD, Harris WH, Ramsey PL, MacEwen GD, editors. The Hip: Proceedings of the third open scientific meeting of The Hip Society. St Louis, MO: CV Mosby;1975. p. 212–228.
22. Tönnis D, Heinecke A. Acetabular and femoral anteversion: relationship with osteoarthritis of the hip. J Bone Joint Surg Am. 1999; 81:1747–1770.
23. Outerbridge RE. The etiology of chondromalacia patellae. J Bone Joint Surg Br. 1961; 43-B:752–757.
24. Lee YK, Ha YC, Hwang DS, Koo KH. Learning curve of basic hip arthroscopy technique: CUSUM analysis. Knee Surg Sports Traumatol Arthrosc. 2013; 21:1940–1944.
25. Neumann M, Cui Q, Siebenrock KA, Beck M. Impingement-free hip motion: the 'normal' angle alpha after osteochondroplasty. Clin Orthop Relat Res. 2009; 467:699–703.
26. Byrd JW, Jones KS. Prospective analysis of hip arthroscopy with 2-year follow-up. Arthroscopy. 2000; 16:578–587.
27. Tanzer M, Noiseux N. Osseous abnormalities and early osteoarthritis: the role of hip impingement. Clin Orthop Relat Res. 2004; (429):170–177.
28. Lage LA, Patel JV, Villar RN. The acetabular labral tear: an arthroscopic classification. Arthroscopy. 1996; 12:269–272.
 XML Download
XML Download