

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Necrotizing fasciitis (NF) is an orthopedic emergency characterized by rapidly progressing necrosis of the fascia and subcutaneous tissue. NF that involves soft tissues needs to be discriminated from cellulitis or abscess, and is difficult to diagnose and manage in its initial stages due to thickening of the subcutaneous fat layer under the skin1). It has a high rate of mortality ranging from 4.2% to 75%, and requires prompt, extensive surgical debridement and appropriate antibiotic therapy2,3). In previous studies, NF was most commonly found to develop unilaterally in a lower limb or hip1,4,5). Fournier gangrene, a form of NF of the perineal region, has been reported primarily in urology and general surgery, but not in orthopedic surgery. Here, we report a case of bilateral NF around the hip that required discrimination from Fournier gangrene in an elderly patient, as the affected area was near the perineal region. Additionally, we also review literature relevant to the current case.
CASE REPORT
A 91-year-old female patient with a chief complaint of a mild febrile sensation and general weakness that lasted for two days was admitted to the emergency room at another hospital. The patient had hypertension controlled by the beta blocker bevantolol, and dementia controlled by donepezil and risperidone. She was able to ambulate and communicate without assistance, although she had limited ambulation after a short-leg splint was placed in order to treat undisplaced fractures of the 4th and 5th metatarsal bones of the right foot two weeks before her emergency room visit. She had no injury with skin defects, trauma history, or injection history. She complained of watery diarrhea starting a week before her emergency room visit, and she started to produce small amounts of sputum over the last two days. The abdominal computed tomography (CT) scan taken in a previous hospital before referral to our hospital revealed fluid retention and a gas shadow in the right gluteal area and around the greater trochanter of the femur. She was transferred to our hospital for intensive care, as sepsis following soft tissue infection was suspected. At the time of the transfer, she had a systolic blood pressure (SBP)/diastolic BP of 149/64 mmHg, a pulse rate of 74 beats/minute, a respiratory rate of 17 breaths/minute, and a body temperature of 36.5℃. Physical examination revealed no evidence of skin necrosis or fluctuation; generation of a mild level of heat was the only finding around the hip and thigh. Her BP subsequently dropped to 81/38 mmHg, her body temperature increased to 38.5℃, and she complained of a chilling sensation.
Laboratory findings included a white blood cell (WBC) count of 14,300/mm3 (normal range: 4,000-10,000/mm3, neutrophils 95%), an erythrocyte sedimentation rate (ESR) of 41 mm/hour (normal range: <20 mm/hour), and a C-reactive protein (CRP) level of 17.46 mg/dL (normal range: <0.5 mg/dL). Under a diagnosis of sepsis, she started to receive the broad-spectrum antibiotics ceftriaxone and clindamycin.
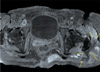
Gas was observed on the right gluteal area on plain radiographs of the pelvis (Fig. 1). Additionally, increased signal intensity was observed along the gluteus fascia to the greater trochanteric area on magnetic resonance imaging (MRI), and abscess formation was identified between the right gluteus maximus and medius (Fig. 2). A smaller abscess was situated on the left gluteus maximus. Air formation was identified, indicating invaded inflammatory lesions on both sides of the hips. Although cystic shadows in the posterosuperior surface of the uterus were detected, radiographic findings were insufficient to determine a connection to the hip lesions.
Based on the aforementioned findings, bilateral NF was confirmed around both hips and hip joints, along with the fascia and muscles, occurring in layers deeper than the skin and the subcutaneous layer. After her BP was stabilized, prompt incisions and thorough debridements were performed on the following day. Taking the patient's comorbid conditions into account, surgery was conducted only on the right side (the side with clear abscess and gas formation) in order to minimize operating time. Surgical procedures were carried out using a posterolateral approach in the right lateral position. No definite skin lesion was detected around the thigh or hip. Bacterial cultures and subsequent identifications were performed on a gray-colored abscess discharged at the time of incision. Abscess and necrotic tissues were observed along the gluteus medius and greater trochanter of the femur. Additionally, deep muscles along with the fascia and subcutaneous tissues were partially invaded. These areas were removed intraoperatively. After sufficient debridement and lavage, the patient underwent a right hip joint puncture for culture tests. A drainage catheter was inserted and the surgical site was sutured. The patient was referred to a gynecologist due to cystic lesions along the superior surface of the uterus, which were considered to be a possible cause of infection. Transvaginal sonography was conducted by switching the patient to the lithotomy position, and puncture and aspiration were performed. The aspirated fluid was clear and lesions were clinically judged to be non-inflammatory. Postoperatively, she was under intensive care for two days with a SBP of 132 mmHg and a body temperature of 36.2℃. She had a WBC count of 9,400/mm3 (neutrophil 95%), ESR of 16 mm/hour, and a CRP level of 3.77 mg/dL. It should be noted that all of these measurements were improved postoperatively.
Escherichia coli was detected by culture tests conducted intraoperatively, and treated with sustained-release ciprofloxacin. The drainage catheter, which had been in place for a week, was removed after tip culture. After managing surgical wounds for two weeks, suture removal was conducted without complications. Subsequently, her ambulation was limited by a combination of sepsis and the trauma of an operation following a rapidly progressive infection. Additionally, a pressure ulcer that occurred on the ischial areas was detected and considered to require management.
General symptoms, high fever, and other findings were not identified after the initial operation. On postoperative day 14, the patient's CRP level was elevated to 8.37 mg/dL with a raised body temperature of 38.5℃. Taking into account possible symptoms caused by her pressure ulcer infection, the patient was followed-up with antibiotic administration. However, a follow-up MRI was performed due to persistently increased body temperature and CRP levels. An increase in the size of the abscess was found between the left greater trochanter and the gluteus medius (Fig. 3). Therefore, incision and debridement were performed on the left aspect. Considering the extent of the necrotic tissues, a wide posterolateral incision was made. No specific pus was noted intraoperatively. Bacterial cultures and subsequent identifications were performed on drained serosanguinous fluid, and the surgical site was sutured after inserting a drainage catheter.
The patient received postoperative care in an intensive care unit and recovered gradually. No bacteria were detected in the culture tests from the second operation. Additionally, her body temperature did not exceed 36.7℃. Further deterioration of the ischial pressure ulcer required wound dressing and care.
She began ambulation using a wheelchair 3 weeks after the second operation. No infection-related complications were observed during a 6-month follow-up. Patient conditions improved substantially with consistent systematic rehabilitation.
DISCUSSION
NF is a rare infection and an orthopedic emergency that requires discrimination from severe cellulitis or abscess. NF is classified into three types according to its causative microbiology. Type I is characterized by synergistic polymicrobial infections caused by non-Group A streptococci, as well as aerobic and anaerobic organisms. Type II involves Streptococcus pyogenes alone or in combination with Staphylococci. Type III is caused by marine Vibrio species after exposure to raw seafood or seawater and marine animals, and is lethal in 30-40% of all cases6). Type I NF, which accounts for more than 70% of all NF infections, is more likely to occur in immune compromised patients, has various prognoses according to patients' underlying diseases, and progresses slower than other types3,4).
The elderly patient in the present case report developed Type I NF that had progressed over 3 days after abdominal symptoms (diarrhea), and the causative pathogen was identified as E. coli. Although only a single strain was identified due to the administration of antibiotics before performing the surgery and culture test, gas formation on plain radiographs and broad necrosis found in the operating room indicated that the infection was caused by multiple microorganisms acting synergistically. Gas tracking and necrotic tissues that spread along the fascial planes on CT imaging are typical clinical features of NF7). Gas was observed only on the right gluteal area on plain radiographs, and the degree of tissue invasion was less severe on the left side as compared to the right on the CT image. However, the patient was diagnosed with bilateral NF around both hips, as a gas shadow and a progressive infection spreading along the fascial planes were observed. Although not all cases of NF show gas formation on plain radiographs, gas is only seen in 3% of non-NF cases as opposed to 32% of NF cases. Thus, detection of gas formation may aid in the early diagnosis of this infection8).
To determine whether the uterine cystic lesions observed during the preoperative evaluation were causing the infection, the patient was referred for assessment by a gynecologist. Results from that assessment confirmed that these lesions were not causative of the infection. Fournier gangrene, a form of NF of the perineal region, commonly requires care and treatment in gynecology, urology, and general surgery departments. In some cases, colostomy can be performed concurrently with surgical debridement to prevent fecal contamination of the surgical wound9). In the present case report, the possibility of Fournier gangrene was excluded after preoperative exams. However, clinical symptoms (a febrile sensation in the hip) were insufficient to discriminate NF from Fournier gangrene. In the case of Fournier gangrene, gynecologist or general surgeon has to treat patient promptly and that will result better prognosis. Although the authors intended to conduct a colonoscopy and examinations of additional organs to clarify the exact cause of the infection, the patient and her family members rejected the procedures. The causes of the serious infection were therefore assessed by evaluating her intraperitoneal organs on the preoperative abdominal CT and MRI, and confirmed intraoperatively.
In a case report described by Kim et al. (2013)5), rectal cancer was confirmed through additional examinations after managing NF around the unilateral thigh. However, unsatisfactory results were obtained due to the refusal of the patient and the patient's family members to undergo aggressive treatment. For patients with NF of the thigh with no exact cause, they suggest a heightened level of clinical suspicion pertaining to abdominal or intestinal causes, and recommend CT scanning.
Unlike the case report by Kim et al.5), the rare condition observed in the present case report, bilateral NF affecting the thigh and hip, has not yet been reported in the literature. Because older patients have a poorer prognosis relative to younger patients, the decision to perform any aggressive treatment in an elderly patient is made more difficult and complicated. Due to the patient's unstable condition at the time of the initial operation in the present case, thorough surgical debridement to shorten the operating time could not be performed. Based on further deterioration of symptoms detected during a follow-up examination, and additional debridement was done on the left aspect.
Prompt diagnosis, thorough debridement, and the use of adequate antibiotics are critical in the treatment of Type I NF. Because this infection is assumed to be polymicrobial, the use of adequate antibiotics is essential for treatment3). The prognosis may be unfavorable in patients ≥60 years of age with diabetes, hypotension, renal failure, and other conditions. Nevertheless, the patient in this case report was able to recover from NF due to prompt surgical management and an interdisciplinary approach to the underlying diseases. The results of a previous study suggested that aggressive surgical intervention reduced a mortality rate of 35% to 4.2%10), and complete debridement is mow recommended instead of removing only nonviable tissues. Additional operations may be warranted in some cases. Although 1-2 sessions of surgery can achieve good results1,4), 3-4 operations are carried out on average6). In addition, appropriate surgical management is critical for infection control.
The elderly patient in the present case report had NF around both hips, and it was difficult to discriminate this patient's signs and symptoms from those of Fournier gangrene, a form of NF of the perineal region near the hip. Prompt radiologic evaluation and systematic management in several departments resulted in favorable outcomes. Despite the necessity of performing debridement separately on each side of the hip, early and aggressive treatment led to recovery from NF, despite the risk imposed by the patient's older age. A better prognosis is expected with thorough debridement of all lesions associated with bilateral NF.


 XML Download
XML Download