

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Obturator (Inferior) dislocation of the hip joint is very rare. There have been some reports of traumatic obturator dislocation of the hip with concomitantly developed osteochondral fracture of the femoral head or greater trochanter1,2,3,4). However, there is no report describing early complications associated with closed reduction of the obturator hip dislocation. In this case report, we present a fracture of greater trochanter during closed reduction of the obturator type hip dislocation. The patient was informed and consented that his case would be submitted for publication.
CASE REPORT
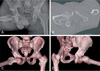
A 47 year-old man was admitted to our emergency department after a motorcycle accident with his right hip in a fixed position of 90° flexion, 90° abduction and externally rotation. The patient had a history of hitting an electric pole with his right thigh with abduction force during collision. The patient complained of severe pain during movement of his right hip joint. His vital signs were stable. There were no neurovascular deficits in the injured limb. An anteroposterior radiograph revealed an inferior, obturator-type dislocation of the right hip joint (Fig. 1A). Computed tomography (CT) scan was performed before any manipulation to evaluate any associated injury. There was no additional damage to the femoral head, acetabulum or trochanteric area (Fig. 1B-D). After appropriate consultations, manipulation under anesthesia was taken.
General anesthesia was administered with patient in supine position. The dislocation was reduced as per the recommended techniques. We applied continuous traction in line with femur with gentle flexion5) and lateral push was given on the inner thigh with the pelvis stabilized by an assistant. However, this was unsuccessful. The hip was then internal rotated and adducted. Forceful resistance was abruptly reduced with audible "clunk" and we checked stability and range of motion of the hip. Reduction of the hip joint was confirmed under fluoroscopy and skin traction was applied for maintenance. Post-reduction CT was taken in order to confirm the congruent reduction. Although the post-reduction X-ray had shown minimal contour change of the greater trochanter (Fig. 2A), post-reduction CT scan revealed the fracture of the greater trochanter (Fig. 2B, C). The authors considered the possibility of further displacement of the greater trochanter, because the fracture gap was more than 2 mm on CT image. The fracture of the trochanter was then fixed through the incision under fluoroscopy control with cannulated screws and washers (Fig. 3A). The patient was discharged with advice for strict bed rest for three weeks, followed by crutch walking for next three weeks. At the final follow-up after two years from trauma, the patient had a pain-free hip joint with active full range of motion (Fig. 3B).
DISCUSSION
The literature has reported very few complications following closed reduction for obturator dislocation of the hip joint, although fracture of the femoral head, neck and greater trochanter or iliac spine1,2,3,4), and open dislocation of the hip joint6) which is concurrent with obturator dislocation have been previously reported. There have been no previous reports describing the early fracture complication of greater trochanter as a result of closed reduction of this type of hip dislocation. However, in case of anterior dislocation of the hip, the neck or greater trochanter of the femur may impinge on the posterior acetabulum rim or ischium7). Therefore, greater trochanter is likely to be weakened and may be more vulnerable to fracture during closed reduction.
Traumatic anterior dislocation can be classified into superior and obturator types. The mechanisms of anterior dislocation are known to be the result of hyperabduction and extension. It has been suggested that anterior dislocations can occur in deceleration injuries like a in car accident which the leg is in a relaxed position with flexed, abducted, and externally rotated during collision, as well as in motorcycle accidents in which the legs are frequently hyperabducted5). The degree of hip flexion is known to determine the type of anterior dislocation, with extension leading to a superior pubic dislocation and flexion resulting in an inferior obturator dislocation5). There are few reports in literature about the technique of reduction8,9), and most authors reported a slight modification of the recommended technique to achieve reduction in their specified cases. We have used these recommended techniques for reducing the hip joint and experienced difficulty in reducing the hip joint even under general anesthesia. Finally, the patient developed a complication in the form of fracture of the greater trochanter.
As described, the fracture is unlikely to be a missed fracture, since the trochanter was normal in prereduction CT scan. One possible mechanism of this fracture is by avulsion force. The bone around the trochanter might have been in contusion state (weakened) by the impact of greater trochanter against the ischium in 90° hip abduction position (Fig. 4). This possible impact for the mechanism of trochanteric injury was suggested by Korovessis et al.1), although in that case the hip joint was not in 90° abduction position. During closed reduction, the attachment of the glutei muscles may have pulled the posterior half of the greater trochanter away from the femur causing the fracture of already weakened greater trochanter. Other possible mechanism of fracture to be mentioned, which should always be avoided, is by too much force enough to cause fracture during reduction maneuver.
Fracture of the greater trochanter can occur during the closed reduction of obturator type dislocation of the hip joint. Surgeons need to be aware of this complication and detailed review of the pre-, post-reduction radiographs including CT scan should be conducted. In addition, excessive force for reduction should be avoided when treating patients with obturator type dislocation of the hip.



 XML Download
XML Download