

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Adhesive capsulitis of the hip (ACH) has also been referred to as "frozen hip"1) or "capsular constriction"2). It was first described by Caroit et al.3) and since then there have only been few publications on the condition4,5,6). However, subsequent experience has led authors to speculate that this condition does exist more commonly than was suggested earlier6). There have been descriptions of case reports of the same but there is a lack of description of a case series. The medical literature has described two kinds of ACH; primary idiopathic adhesive capsulitis of hip (IACH) and secondary ACH2,6). They have defined IACH as adhesive capsulitis that is present without known etiology or concomitant pathology. If adhesive capsulitis was present secondary to pathology it was defined as secondary. Little has been described in literature concerning IACH. Its presentations can be challenging and does require further diagnostic testing. The clinical suspicion of IACH involves restricted range of movement and normal hip radiographs. This presentation is similar to that for adhesive capsulitis of the shoulder (ACS)3). ACH is due to retraction of the fibrous joint capsule of the hip and unless IACH is diagnosed through surgery or biopsy, clinicians must rely on the patient's history and clinical findings and normal radiography to diagnose IACH5). There is a lack of description of an objective evaluation modality that demonstrates direct evidence of this. Thus the purpose of this study was to delineate the characteristic of findings observed on magnetic resonance arthrography (MRA) by identifying the capsular thickness involved and their significance on clinical presentation of restricted range of motion in cases with IACH and to report on the authors experience with the diagnosis of IACH.
MATERIALS AND METHODS
From September 2006 to August 2012, MRA images of all the patients with hip pain or restricted range of movements, with normal plain hip radiographs were retrospectively assessed.
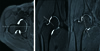
At the time of this reporting, the database consisted of 46 hips (44 patients). We excluded all subjects who have soft tissue abnormal (labral tear or ligament tear 16 hips). Out of them, 10 hips (8 patients) were selected in the study group (Table 1), who were diagnosed as cases of IACH by the evaluation of a single radiologist on MRA findings. Diagnostic criteria of IACH which we assuming are as 1) reduction of intra-articular capacity of joint, 2) limitation of range of motion, with or without pain. Twenty patients were included in the control group with normal MRA findings and with only hip pain without limitation of range of motion. Rests of the cases were excluded from the study (Fig. 1). The exclusion criteria were abnormal laboratory result (blood cell count, inflammation markers, blood phosphate/calcium balance), in the presence of any sign of osteonecrosis or progressing coxarthrosis by radiological examination, inflammatory arthritis (rheumatoid arthritis, systemic lupus erythematosus etc.) excluded secondary ACH. The study group included 10 hips (8 patients) with 3 males and 7 females. The average age of the patients with IACH was 44.4 (28-64) years. The average duration of symptoms was 8 (2-24) months. The control group included 20 hips (20 patients) with 7 males and 13 females. The average age of the patients was 47.1 (21-72) years (Table 2). The restriction of motion, which was initially recorded by a single senior surgeon was noted and compared for the study group and control group (Table 3). A single radiologist recorded the MRA finding of IACH. The MRA images of the patients in the study group were assessed; T1 weighted image was chosen where the femur head was the widest and coronal cut was taken at the center of the femur head (Fig. 2A). The capsular thickness was measured in the anterior and posterior and inferior recess as shown in Fig. 2B. Similarly, T1 weighted images showing femur head as widest was cut in the axial plane at the center of the femoral head (Fig. 3A). The capsular thickness was measured in the superior and inferior recess as shown in Fig. 3B. And three surgeons independently measured capsule thickness to evaluate the interobserver variability (intraclass correlation coefficient, 0.853). All patients with IACH received conservative therapy, but patient who unrelieved the symptoms by conservative treatment, in whom arthroscopic release was performed. Conservative treatment included lifestyle modifications to avoid pain-provoking activities, supervised physical therapy, and oral anti-inflammatory medications.
The statistical analysis was performed to compare the differences between the two groups. An independent Student t-test and Wilcoxon rank-sum test were using SPSS Statisics software (for Windows Release ver. 17.0; SPSS Inc., Chicago, IL, USA), and significance was accepted at the 95% level. P-values of less than 0.05 were considered significant.
RESULTS
The range of motion possible was recorded in flexion, abduction, adduction, external rotation and internal rotation. In the control group, the mean flexion was 136.7°±5.9°; mean abduction was 42°±4.9°; mean adduction was 31.5°±2.8°; mean external rotation was 41°±3.4°, mean internal rotation was 36°±3.4°. For patients in the IACH group the mean flexion was 122.5°±5.5°; mean abduction was 28°±2.8°; mean adduction was 26.5°±2.4°; mean external rotation was 30.5°±3.8°, mean internal rotation was 25.5°±2.4°. There was a statistically significant reduction in the mean range of motion of hip joints in all planes, in patients of the IACH group when compared with the control group. However, even though there was global restriction of motion in the hip joint, the patient complained of maximum restriction in range of rotation (Table 3).
The capsular thickness was measured on the MRA in millimeters as described earlier, in the anterior, posterior, superior and inferior recess. The mean capsular thickness in the control group was 2.61±0.8 mm anteriorly, 1.94±0.5 mm posteriorly, 1.88±0.5 mm superiorly and 1.84±0.5 mm inferiorly. Similarly, the mean capsular thickness in the IACH group was 3.14±0.7 mm anteriorly, 2.61±0.5 mm posteriorly, 2.78±0.5 mm superiorly and 2.13±0.4 mm inferiorly. The capsular thickness showed statistically significant difference between the control and IACH groups in the posterior and superior recess (Table 4).
DISCUSSION
Caroit et al.3) introduced the concept of ACH. Since then only a dozen or so articles have been published referring to this diagnosis1,2,3,5,6,7,8,9,10,11,12). Adhesive capsulitis of a joint has been defined as a condition that begins with synovial inflammation and ends in capsular fibrosis13,14,15,16). The fibrosis of joint capsule in IACH is caused by the same cytokines as that for ACS; however, their levels vary. Hsu et al.17) has reported the association between ACS and IACH, but this has not been previously discussed in the literature in details. Presently, there is no study that has examined or that can pinpoint the changes that occur, in otherwise unexplained IACH.
The exact reported incidence of ACH is unknown but it is probably higher than is generally thought. It is said to selectively affect women between the ages of 35 and 501,3,6,18). In our study seven out of ten patients, of the IACH group were middle-aged women ranging in age from 31 to 61 years. Six out of the ten patients had other co-morbid medical conditions typically associated with adhesive capsulitis like diabetes mellitus, hypertension and hyperlipidemia. Patients suffering from diabetes mellitus have shown to have tendency to develop IACH, associations have been established in similar involvement for the shoulder2,19). However this cohort is too small to draw any reliable conclusions on this aspect.
For the diagnosis of IACH clinicians have mostly relied on their clinical findings, unless it is diagnosed through surgery or biopsy6). Literature shows that in the diagnosis of IACH, hip radiographs often reveal only osteopenia. The other tests also are most often negative5). Radiographic abnormalities have generally been reported only when there is underlying disease that leads to adhesive capsulitis2,7). In this study the radiographs of the hip were normal in all the 10 hips and this is consistent with the literature. Magnetic resonance imaging (MRI) and computed tomography criteria for ACS have been well known3,11,18,20). Similarly, authors6) also suggest role of MRI of the hip in order to detect potential bone or cartilage pathologies. Although some authors2,7) have described observations of tightness during arthrography as sign of reduced articular capacity and adhesive capsulitis, others have only argued of its relevance for IACH. Studies have also pointed out the need for a contra-lateral injection to compare and validate results6).
And MRI can show evidence of capsular fibrosis where there is thickness of the anterior joint capsule11). But the literature only evaluated axial view in MRI. So best to our knowledge the characteristic of MRA for IACH has not been described in literature yet.
In ACH, there is limitation of motion in all three planes (flexion-extension, internal-external rotation and abduction-adduction)3,6). Some authors suggest that IACH is under-diagnosed as it leads to less functional limitation as compared to the other joints, loss of range of motion is much better tolerated in the hip than other joints, such as the shoulder and knee3,12). Similar results were observed in our study that the range of motion of the hip joint in the patients with IACH was statistically significantly restricted in flexion, abduction, adduction and rotations. However, the patient complained mainly of loss in motion.
The limitation of this study is its retrospective design and small sample size. Future studies are needed with larger sample size and longer follow-up. And we could not compare to contralateral normal hips of the IACH patients due to 2 patients have both hip problem. If we compare contralateral normal hip of the IACH patients, we would have been excluded to differences in individual difference in thickness of the capsule. And we did not distinguish between each stage of IACH like an ACS22), because there was no proven or disproved by definitive diagnostic test like histopathology or arthroscopic finding. So In order to make an accurate diagnosis of IACH need to histopathology or arthroscopic finding.
CONCLUSION
In summary, IACH is a clearly identifiable entity. The clinical presentations are similar to those commonly attributed in the shoulder. The principal clinical finding is painful restricted motion especially rotations. There is a predilection for middle-aged women. The characteristic of MRA is to identify the presence and location of capsular thickening superiorly and posteriorly, which correlates clinically as restricted motions. And there change in the capsular thickness can be helpful in further surgical treatment.






 XML Download
XML Download