

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Mechanical symptoms of the hip such as clicking, locking, and giving way are well known to be related to bony structural abnormalities of the femur or acetabulum and combined femoral and acetabular bony abnormalities. These structural abnormalities are called femoroacetabular impingements (FAI) and are classified as the cam-type, pincer-type, or combined-type. FAI has recognized to predispose acetabular labral tears and chondral damage, and the subsequent development of osteoarthritis3,8).
To understand bony structural abnormalities in patients with those mechanical symptoms, plain radiography, magnetic resonance imaging (MRI) with and without arthrography, and computed tomographic arthrography (CTA) have been advocated for the assessments of morphological abnormalities. Plain radiograph is simple and straightforward to analyze, but the projection of the beam and patient position can cause measurement inaccuracies1,5,7,24). In almost all of the previous studies, magnetic resonance arthrography (MRA) has been considered the gold standard for the assessment of bony structural abnormalities and associated abnormalities, such as, labral tears, cartilage damage, and loose bodies. In addition, advantages of MRA are superior soft tissue contrast and capacity to depict fine anatomic detail and increase diagnostic accuracy. However, MRA has some limitations; in particular, it involves lengthy examination times and has relatively low spatial resolution, which makes the detection of very small structures and bony structural abnormalities difficult4). On the other hand, computed tomography (CT) has high accuracy for the detection of bony structural abnormalities and tendon and labral calcifications4,6). In addition, multi-detector CT arthrography (MDCTA) provides multiplanar images of lesions, which are comparable to MRA images, and MDCTA allows the reconstruction of images with a section thickness of 1 mm or less in any direction in target lesions. Accordingly, the isotropic data acquisition and the high spatial resolution of MDCTA are required for the accurate imaging of morphological abnormalities of the hip joint.
In the studies which reported labral lesions and bony structural abnormalities, it has been discovered acetabular labral tears rarely occur in the absence of a structural osseous abnormality17,22). However, relationships between mechanical symptoms and bony structural abnormalities have rarely been studied, and no study has yet compared the symptomatic hips with asymptomatic hips regarding structural bony abnormalities.
Accordingly, this retrospective study was conducted to determine the difference in prevalences of structural bony abnormalities in patients with and without mechanical symptoms of the hip joint and to determine mechanical symptoms of hip joint are related to the presence of structural bony abnormality and the prevalence of structural bony abnormalities in symptomatic patients diagnosed to have a labral tear using MDCTA.
MATERIALS AND METHODS
The design and protocol of this retrospective study were approved by the institutional review board of each hospital. All patients were informed that their medical data could be used in a scientific study and have provided consent.
Between November 2007 and April 2010, 151 patients (151 hips) who had complained of mechanical symptoms and positive impingement, underwent MDCTA. Indications for MDCTA were a complaint of a mechanical symptom, such as clicking, locking, or giving way for minimum of 3 months, and a positive sign by physical examination, including impingement test, log-roll test, FABER test, or Patrick test. There were 68 men and 83 women of mean age at the time of diagnosis of 44.8 years (range, 16-73 years) (Table 1). The 151 asymptomatic subjects were matched with the 151 symptomatic subjects for gender, age (within one year), site (right or left), and time of CT examination (within 6 months). The indications of control group were pain coming from a ureter stone and a diagnostic abdominal and pelvic CT scan. We confirmed that the control group did not have any history of hip-related mechanical symptoms through a simple questionnaire and individual interview.
1. Imaging Protocols
1) Computed tomographic arthrography
Under fluoroscopic observation in a supine position, a 22-gauge needle was inserted just below the femoral head at the head and neck junction. The needle tip was placed inside the affected hip joint at the femoral head-neck junction to minimize the likelihood of damage to the acetabular labrum or articular cartilage, and 10-12 mL of meglumine ioxitalamate-saline solution (13 mL meglumine ioxitalamate [Telebrix 30 Meglumine; Guerbet, Aulnay-sous-Bois, France] in 7 mL of normal saline) was injected. CT scans were obtained with a 16-channel (Mx 8000 IDT; Philips Medical Systems, Best, Netherlands) or a 64-channel multi-detector CT system (Brilliance 64; Philips Medical Systems) using the following standard acquisition protocols. For 16-channel MDCT; rotation speed 0.75 seconds per rotation, 240 mAs, 120 kVp, a collimation of 2.5 mm, field of view at acquisition 15 cm, slice thickness 1.0 mm, and a slice increment of 0.5 mm (50% section overlap). For 64-channel MDCT; rotation speed 0.75 seconds per rotation, 300 mAs, 140 kVp, a collimation of 0.625 mm, field of view at acquisition 30 cm, slice thickness 0.67 mm, and a slice increment of 0.33 mm (50% section overlap). This high-resolution isotropic CT volume allowed image reformation in any desired plane without degrading image quality. Routinely, coronal, sagittal, and oblique axial images (parallel to the femoral neck axis) were reconstructed using Rapidia 2.8 workstation (Infinitt, Seoul, Korea) after axial scanning.
2) Computed tomography reformations in the control group
Raw data from the abdominal and pelvic CT scans performed on a 16-channel (Mx 8000 IDT) or 64-channel multi-detector CT system (Brilliance 64) using standard acquisition protocols, were reformatted using a bone algorithm as follows: (1) orthogonal axial plane through the pelvic and hip joints; (2) oblique coronal and axial planes along the plane of the femoral neck for each hip; (3) transparent 3-dimensional (3D) rotational model of the whole pelvis (simulating a pelvic radiograph), allowing anterior/posterior and lateral rotation; and (4) 360° rotational 3D model along the axis through the center of the femoral neck for each hip (Fig. 1).
2. Anatomic assessments important for normal biomechanical function
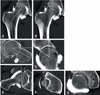
Femoral neck shaft angle, lateral center-edge angle, anterior center-edge angle, cranial and central acetabular version, and alpha angle were measured by MDCT (Fig. 2).
For the measurement of femoral neck shaft angle, lateral center-edge angle, anterior center-edge angle, and central acetabular version, we have used a plane which goes through the center of both femoral heads. For the measurement of cranial acetabular version, we have use a plane that passes through at a point corresponding to the 1 o'clock position of both femoral head.
To minimize measurement errors in assessment of acetabular orientation and femoral head coverage, we have standardized the position of the pelvis in relation to the rest of the body at the time of measurement by adjusting the vertical plane to the anatomic position of the pelvis.
Femoral neck shaft angles described by Tönnis19) were measured at the midcoronal section of MDCT. The normal range of femoral neckshaft-angle is 125°-135°. Coxa vara is defined as a measurement of <125°and coxa valga as one of >140°19). Lateral center-edge angles were measured using the method devised by Wiberg23). The center-edge angle is normally >25°; an angle of 20°-25° is considered borderline23) and a one of >39° is considered as overcoverage20). Anterior center-edge angles were measured using the method devised by Lequesne and Sèze11). The center-edge angle is normally >20°. Acetabular version was measured using the method devised by Reynolds et al.18), who classified acetabular version as cranial and central acetabular version. Cranial acetabular version angles were measured at a point corresponding to the 1 o'clock position on the femoral head, and a measurement of <0° was considered to indicate retroversion18). Central acetabular retroversion was measured at a point corresponding to the 3 o'clock position on the femoral head, and a measurement of <10° was considered to indicate retroversion18). Alpha angle developed by Nötzli et al.15) was used to determine the femoral head-neck junction and were considered abnormality when >50°. This method which originally developed on MRI was transferred to MDCT examination16).
3. Statistical analysis
Two blinded reviewers (JJH and JHM) independently reviewed the MDCT scans of the 151 symptomatic patients on two separate occasions. There was no communication between the two reviewers. MDCT data was presented in a random order and the orders were changed in the two different sessions. We assessed interobserver and intraobserver reliabilities in the six measured parameters including neck shaft angle, lateral and anterior center edge angle, and cranial and central anteversion using interclass correlation coefficients. Intraclass correlation coefficients were interpreted as follows: <0.20, slight agreement; 0.21-0.40, fair agreement; 0.41-0.60, moderate agreement; 0.61-0.80, substantial agreement; and >0.80, almost perfect agreement12). Kappa coefficients were also used to assess the reliabilities of labral abnormality, and were interpreted as follows; <0.00, poor agreement; 0.00-0.20, slight agreement; 0.21-0.40, fair agreement; 0.41-0.60, moderate agreement; 0.61-0.80, substantial agreement; and >0.80, almost perfect agreement10).
Femoral neck shaft angles, lateral center-edge angles, anterior center-edge angles, cranial and central acetabular versions, and alpha angles were also measured in the symptomatic and asymptomatic groups to be compared.
The chi-square test was used for categorical variables and the t-test for numerical variables. All reported P-values were two sided, and P-values of <0.05 were deemed significant. The results were expressed as odds ratio (OR) with 95% confidence intervals (CI) for the symptomatic group relative to asymptomatic group. Data were analyzed statistically using SPSS program ver. 12.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
One hundred and twenty one of the 151 symptomatic hips (80.1%) had a structural bony abnormality and 107 hips (70.9%) a labral tear. One hundred and forty-three (94.7%) of the 151 symptomatic hips had a structural abnormality and/or labral tear.
Thirteen hips (10.7%) of 121 structural bony abnormalities in symptomatic hips were the isolated cam type (alpha angle >50°), 3 hips (2.5%) had dysplasia (lateral center edge angle [CEA] <20°), 89 hips (73.6%) were the isolated Pincer type (lateral CEA >39° or cranial acetabular retroversion <0° or central acetabular retroversion <10°), and 16 hips (13.2%) were the combined type. Of these 121 hips, 51 (42.1%) had one structural abnormality, 43 (35.5%) had 2 structural abnormalities, 20 (16.5%) had 3 structural abnormalities, and 7 hips (5.8%) had 4 structural abnormalities.
Eighty-two of the 151 asymptomatic hips (54.3%) had a structural bony abnormality. Six (7.3%) of these 82 structural bony abnormalities were of the cam type, 4 hips (4.9%) had dysplasia, and 72 hips (87.8%) were of the pincer type, but no hip was of the combined type. Sixty-five hips (79.2%) in the asymptomatic group had one structural abnormality, 13 hips (15.9%) had 2 structural abnormalities, and 4 hips (4.9%) had 3 structural abnormalities.
The prevalence of patients with at least one structural bony abnormality in symptomatic and asymptomatic groups was 80.1% (121/151) and 54.3% (82/151), respectively (OR: 3.39, 95% CI: 2.30-5.66; P<0.001). Significant differences were found between the symptomatic and asymptomatic groups with regard to neck shaft angle (OR: 3.69, 95% CI: 1.44-9.47; P=0.004), cranial retroversion (OR: 1.81, 95% CI: 1.05-3.10; P=0.031), central retroversion (OR: 9.68, 95% CI: 5.04-18.57; P<0.001), and alpha angle (OR: 5.26, 95% CI: 2.10-13.16; P<0.001). However, no significant intergroup differences were found on lateral center edge angle (P=0.094) or anterior center edge angle (P=0.156) (Table 2).
In subgroup analysis of labral tear group in symptomatic patients, 85 (70.2%) of the 121 hips with a structural bony abnormality had a labral tear according to MDCTA. Eighty-six (80.3%) of the 107 symptomatic hips with a labral tear had a structural bony abnormality and 36 (81.8%) of the 44 symptomatic hips with a normal labrum had a structural bony abnormality (P=0.559). Twenty-one (19.6%) of the 107 symptomatic hips with a labral tear had a normal bony structure. Age (P=0.478) and structural bony parameters, including alpha angle (P=0.143), lateral CEA (P=0.481), cranial (P=0.746) and central (P=0.715) acetabular anteversion (P=0.507), neck shaft angle (P=0.135), and anterior CEA (P=1.000), were no different in the two study groups (Table 3).
Intra- and inter-observer correlations for combinations of all measurements were found to be reproducible and reliable among observers.
DISCUSSION
In the present study, we compared neck shaft angles, lateral and anterior center edge angles, cranial and central acetabular versions, and alpha angles to identify structural bony abnormality in hips with and without mechanical hip joint symptoms. This study demonstrates that the rate of structural bony abnormality was significantly greater in the symptomatic group than in the asymptomatic group (80.1% vs. 54.3%). All six measured parameters differed in the two study groups, which supports our hypothesis that mechanical symptoms are related to the presence of a structural bony abnormality or of a labral tear. In addition, morphologic signs of impingement were more frequent in the symptomatic group.
No previous comparative study has been conducted on structural bony abnormalities in patients with mechanical symptoms. Recently, Weir et al.21) performed a radiologic assessment of FAI in 68 hips presenting long-standing adductor related groin pain. They demonstrated that 94.1% (64/68) of assessed symptomatic hips had shown radiological signs of FAI21). Beaule et al.2) compared alpha angles of 36 painful non-dysplastic hips (30 patients) and 20 asymptomatic hips (12 patients) using 3D computed tomography, and found cam type deformity (alpha angle >50°) in 70% of symptomatic patients and in 10% of asymptomatic controls. To date only one study has reported the prevalence of abnormalities in an asymptomatic population. Kang et al.8) assessed 50 patients (100 hips) with no history of hip problems in relation to FAI using CT, and demonstrated that only 39% of hip joints had at least one morphologic aspect predisposing FAI8). This finding concurs with our finding of a structural bony abnormality in 54.3% of asymptomatic patients.
Structural bony abnormalities were classified as either the cam or pincer type. Cam and pincer impingements are known to occur rarely in isolation. In one epidemiological study with 149 hips having impingement, 17% had isolated cam impingement, 10% had isolated pincer impingement, and 72% had combined cam-pincer impingement3). In the present study, of 121 hips with a structural bony abnormality in symptomatic patients, 75% had an isolated pincer type, 10.7% had an isolated cam type abnormality, and 13.2% had combined cam-pincer impingement. These differences between studies could be due to the differences in methods used for subject selection, the applied diagnostic criteria, gender, and ethnicity and the age of study subjects9).
This study has several limitations that require consideration. First, this was a retrospective matched case-control study, and selection bias might have been introduced when we chose members of the asymptomatic group. Probably, underestimate non-response individuals. However, when selecting these controls, after questionnaire we interviewed them individually and confirmed an asymptomatic hip joint condition. We thus believe that control selection does not diminish our finding that mechanical symptoms are rarely seen in the absence of a structural bony abnormality. Second, the results of this study are difficult to compare directly with those of other studies, since the different methods were used to measure parameters, and the different diagnostic criteria were used within different cohorts. However, the prevalence of a structural abnormality in the symptomatic and asymptomatic groups that was found during the present study show similar trends to those found previously2,8,13). Third, we did not confirm the presence of a labral tear surgically. Recently, two studies have demonstrated that CTA provides an excellent means of detecting labral lesions (the sensitivity, specificity and accuracy of CTA, using arthroscopic findings as a reference, were 92-97%, 87-100%, and 92-95% for labral tears, respectively)14,25).
Despite these limitations, we have achieved our aim, which was to document the prevalence of bony abnormalities predisposing FAI in symptomatic and asymptomatic individuals.




 XML Download
XML Download