

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Avascular necrosis (AVN) of the femoral head is a disease that affects younger patients (age range usually from 15 to 50 years), and which leads to debilitating arthritis often requiring total hip arthroplasty (THA) for disabling pain. However, neuromuscular diseases, such as, cerebral palsy and poliomyelitis, are a concern in patients with THA, because dislocation frequently occurs after surgery1,2). AVN of the femoral head in a patient with poliomyelitis has only been reported once in the English literature3). Here, we report a case of femoral head AVN in a patient with poliomyelitis, who was treated with a large diameter femoral head metal-on-metal THA using a modified minimally invasive (MI)-2-incision technique4,5). The patient was informed that case data would be submitted for publication, and provided consent.
Case Report
A 59-year-old male presented at our clinic complaining of right hip pain of 2 months duration. When he was 5 years old, he had contracted poliomyelitis and the right side of his body continued to show motor weakness (his upper extremity motor grade was normal but his lower extremity was only fair to good). The left side of his body showed normal motor power, but his left ankle showed adduction, supination, and inversion deformities. Nevertheless, despite the right lower extremity motor weakness and the left ankle deformity, he had been able to walk with a cane. However, after the right hip pain developed, he required a wheel-chair. He was a heavy alcohol drinker without a trauma or a steroid usage history. A physical examination of the right hip revealed a mild range of motion limitation (flexion 100°, external rotation 40°, internal rotation 5°, abduction 30°, adduction 20°), and a positive Patrick test. Regarding right leg motor power, hip flexion was good, knee extension fair, hip abduction poor, and ankle dorsiflexion and plantar flexion were poor. He had scoliosis with a fixed right pelvic obliquity and a Trendelenburg gait (Fig. 1).
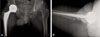
Radiography revealed a sclerotic line at the periphery of the right femoral head and a crescent sign (Fig. 2). MRI of the hip showed a huge right side femoral head AVN lesion with a double line sign and left femoral head had no specific bony signal change. We decided on THA to manage the hip pain, and to prevent dislocation after operation due to abductor weakness we decided to perform a surgery of modified minimally invasive (MI)-2-incision THA4,5) with large diameter femoral head metal-on-metal articulation. The muscle plane was distinguishable despite muscular fatty degeneration and because of fixed pelvic obliquity, the surgeon undertook to increase the lateral opening angle of the acetabular cup to 55°. A cementless acetabular cup (Magnum®, Biomet, Bridgend, South Wales, UK) with a modular 44 mm head, and a cementless femoral stem (M/L taper®, Zimmer, Warsaw, USA) was used. Postoperatively tolerable weight bearing ambulation was allowed with a walker and range motion exercise was encouraged on the first postoperative day.
The patient was discharged at 12 days postoperatively without any complication. He was followed for 2 years, and his walking ability improved to ambulation with a cane (Fig. 3). The follow-up was uneventful, and in particular, no dislocation of the right hip occurred.
Discussion
AVN of the femoral head often occurs after trauma, chronic alcohol consumption or steroid usage, or after diver's disease. However, in many cases it is idiopathic6). In the described case, the patient was assumed to have developed AVN of the femoral head due to alcohol abuse, because he had no other risk factor. As far as we were able to determine, the treatment result with THA in AVN of the femoral head affected with poliomyelitis has been reported only in one patient in the English literature3). Because poliomyelitis mainly affects the anterior horn cells of the spinal cord, sensation is intact and intelligence is unaltered, and thus, our patient was able to carry out our instructions after THA.
Neuromuscular diseases, such as, cerebral palsy, poliomyelitis, and hemiparesis, are of concern when THA is contemplated, because muscle imbalance increases the risks of cement loosening and hip dislocation. The incidence of hip dislocation after THA in patients with neuromuscular disease is unknown, because it is not the procedure of choice in these patients. Frackler and Poss2) reported higher than normal dislocation rates for neuromuscular and cognitive disorder patients. They considered muscle weakness, imbalance, and an inability to comply with activity restriction to be causative factors. Cabanela and Weber1) classified neuromuscular diseases into two categories, those associated with reduced muscle tone, such as, poliomyelitis, Down syndrome, and myelomeningocele, and those associated with increased muscle tone, such as, cerebral palsy, Parkinson's disease, and stroke. In this previous study, 5 THAs were introduced contralateral to hips affected by poliomyelitis, and postoperative results were described to be similar to those of the general population. Furthermore, it was postulated by the authors that reduced activity levels contributed to these results. Spinnickie and Goodman7) reported a case of dissociation of the femoral head and trunion after constrained THA in poliomyelitis with intertrochanteric nonunion, which they revised to a 40 mm femoral head and a non-constrained liner with a 15° elevated lip. In our case, a large modular 44 mm metal head was used because large head metal-on-metal systems are stable and offer a wide range of motion due to a larger femoral diameter (≥38 mm).
Although metal-on-metal bearing results high levels of cobalt and chrome ions found in the blood stream and urine, and pseudotumours, we thought the risk reduction of dislocation was the main issue in this patient. On the other hand metal-on-metal bearings with a larger femoral head size decrease friction and improve the lubricative features of the prosthesis, which improve abrasion resistance8). Another option for bearing with large diameter head is a ceramic articulation (≤40 mm). But ceramic articulation needs more exact acetabular cup positioning and otherwise, squeaking and ceramic fracture can be developed.
According to a recent meta-analysis of 12,203 THA procedures, the dislocation rate of the posterior approach is 3.23% as compared with 2.18% for the anterolateral, 1.27% for the transtrochanteric, and 0.55% for the direct lateral approaches. Thus, in terms of the risk of dislocation, the posterior approach is of greatest concern8). On the other hand, Palan et al9). concluded that dislocation rates after the anterolateral and posterior approaches are similar, and postulated that head size is related to dislocation rate.
MI-2-incision THA was introduced several years ago, and its alleged advantages, which are attributed to no muscle detachment or tenotomy during the surgical approach, are a low dislocation risk and rapid rehabilitation10). Accordingly, we considered that the MI-2-incision THA could be utilized in our patient to minimize of muscle damage to already jeopardized muscles.
Summarizing, THA appears to be a good treatment option for AVN of hips affected by poliomyelitis. However, additional efforts, such as, the use of a large femoral head and a minimally invasive technique, are required to prevent dislocation.


 XML Download
XML Download