

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
The purpose of this study is to evaluate the efficacy of the trochanter reattachment device (TRD) as a firm internal fixation method for bipolar hemiarthroplasty in unstable intertrochanteric femur fracture for elderly patients over 65 years old.
Materials and Methods
From September 2010 to April 2011, 19 patients (M/F: 1/18) over 65 years old were treated with bipolar hemiarthroplasty using the TRD as a fixation method for intertrochanteric femur fracture with above Evans-Jensen classification 2nd (above AO/OTA A1.3). They were followed up for more than 12 months(12-29 months).
Results
Out of 19 patients, only one had loosening of the TRD plate and reoperation was performed. There was no dislocation after surgery. Complete fracture union was observed in 19 patients with follow up of more than 12 months.
Conclusion
In bipolar hemiarthroplasty for intertrochanteric femur fracture, TRD produced easy and firm fixation. Additional fixation with TRD restoring abduction force by union of greater trochanter can be a good choice of surgery for avoidance of dislocation and chronic pain due to trochanteric nonunion after arthroplasty.
Figures and Tables
 | Fig. 1(A) AO TRD (AO Trochanteric reattachment device). It is very important to plan the direction from which the cables will be tensioned. (B) The TRD is also available in a large version. The large TRD is indicated when an additional femur shaft fracture occurred. (C) Applied small TRD at greater trochanter. (The source of image is Synthe® The Cable system for orthopedic trauma surgery).
|
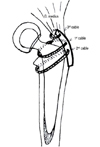 | Fig. 2Schematic procedure sequence. Schematic figure for fixation technique of trochanter with TRD. 1st cable should be placed at neck of stem for firm fixation while tightening. And then, place 2nd cable under the lesser trochanter. 3rd cable should be placed inferior portion of gluteus medius, use tensioner and cable crimper to tighten the TRD at greater trochanter.
|
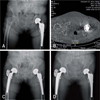 | Fig. 3(A) Bipolar hemiarthroplasty was performed in left hip joint of the patient 2 years ago. On simple x-ray, minimal comminuted intertrochanteric fracture was found at right femur. Large size bone loss of left greater trochaneric area was found. (B) Comminuted fractures and displacement were found on computed tomography. Cemented bipolar hemiarthroplasty was performed in right femur intertrochanteric fracture, and additional fixation using AO TRD was done to comminuted and displaced fracture of greater trochanter and lesser trochanter. (C) Radiograph at 1 year shows bony union of right femur greater trochanter. (D) Compared to left trochanteric bone loss, most bone density is remained at right trochanter.
|

References
1. Barnes B, Dunovan K. Functional outcomes after hip fracture. Phys Ther. 1987; 67:1675–1679.

2. Davis TR, Sher JL, Horsman A, Simpson M, Porter BB, Checketts RG. Intertrochanteric femoral fracture. Mechanical failure after internal fixation. J Bone Joint Surg Br. 1990; 72:26–31.
3. Kyle RF, Gustilo RB, Premer RF. Analysis of six hundred and twenty-two intertrochanteric hip fracture. J Bone Joint Surg Am. 1979; 61:216–221.
4. McKinley JC, Robinson CM. Treatment of displaced intracapsular hip fractures with total hip arthroplasty: comparison of primary arthroplasty with early salvage arthroplasty after failed internal fixation. J Bone Joint Surg Am. 2002; 84-A:2010–2015.
5. Kang CN, Kim JO, Kim DW, Koh YD, Ko SH, Lee KW. Comparison of hemiarthroplasty and compression hip screw on elderly unstable intertrochanteric fractures. J Korean Soc Fract. 1997; 10:738–745.
6. Kim WY, Han CH, Park JI, Kim JY. Failure of intertrochanteric fracture fixation with a dynamic hip screw in relation to pre-operative fracture stability and osteoporosis. Int Orthop. 2001; 25:360–362.
7. Jensen JS. Classification of trochanteric fractures. Acta Orthop Scand. 1980; 51:803–810.
8. Bal BS, Maurer BT, Harris WH. Trochanteric union following revision total hip arthroplasty. J Arthroplasty. 1998; 13:29–33.
9. Dall DM, Miles AW. Re-attachment of the greater trochanter. The use of trochanter cable-grip system. J Bone Joint Surg Br. 1983; 65:55–59.
10. Kim WY, Shin ES, Moon CY. Modified double tension band wiring for reattaching the greater trochanter when performing hemiarthroplsty for intertrochanteric fracture in elderly patients. J Korean Hip Soc. 2009; 21:257–262.
11. Kho DH, Shin JY, Kim KH, Lee JH, Kim DH. Trochanteric management for unstable intertrochanteric femoral fracture in the elderly patients. J Korean Fract Soc. 2007; 20:129–134.
12. Hamadouche M, Zniber B, Dumaine V, Kerboull M, Courpied JP. Reattachment of the ununited greater trochanter following total hip arthroplasty. The use of a trochanteric claw plate. J Bone Joint Surg Am. 2003; 85-A:1330–1337.
13. Chapman CB, Herrera MF, Binenbaum G, et al. Classification of intertrochanteric fractures with computed tomography: a study of intraobserver and interobserver variability and prognostic value. Am J Orthop (Belle Mead NJ). 2003; 32:443–449.
 XML Download
XML Download