

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Distalization of the maxillary dentition has been recognized as an important treatment approach for the correction of Class II malocclusions and it has been traditionally performed using headgear. However, known disadvantages of headgear appliances include poor esthetics and dependence on patient compliance.12 In an attempt to overcome the limitations of headgear, several noncompliance devices such as distal jet and pendulum appliances were introduced.34 However, they often resulted in undesirable side effects such as extrusion and protrusion of the maxillary anterior teeth and extrusion, distal tipping, and distal rotation of the maxillary first molars.56
The advent of temporary anchorage devices (TADs) has allowed better control over unwanted reciprocal movement of the anchor units, although miniscrew insertion in the interradicular region is associated with serious limitations, including a short range of action, coupled with the risk of root injury. Miniplates have been advocated as an alternative to avoid contact with adjacent roots in the area of insertion; however, their placement and removal require more invasive surgical procedures.
Anatomically, the palatal area provides easy access, ample keratinized tissue, and adequate bone thickness and density for the placement of TADs.78910 The modified C-palatal plate (MCPP) has been reported to result in successful distalization of the maxillary dentition without significant side effects in adolescents.1112 In addition, it was recently reported that MCPPs and headgear resulted in similar sagittal skeletal and dental treatment effects in growing patients.13 Moreover, one study demonstrated that MCPPs can be used for maxillary distalization in adults14; however, it was a single-arm study and did not compare the treatment effects of MCPP with those of other conventional devices. Such a comparison can provide a deeper insight into differences in treatment outcomes between appliances and allow for the determination of precise indications for each device on the basis of efficiency and side effects.
Even though the application of headgear in adults may not be very popular, they are widely used as appliances of choice for distalization of the maxillary dentition in patients with Class II malocclusion. Park et al.15 compared the effects of high-pull headgear with those of sliding mechanics aided by the concurrent use of miniscrews in adults. Other studies compared treatment outcomes between headgear and miniscrews or miniplates placed in maxillary posterior region in adults.161718 In 2015, Chen et al.19 used headgear in adult patients with bimaxillary protrusion and compared the treatment effects with those of self-ligation brackets coupled with miniscrew anchorage.
In the aforementioned studies, headgears were mainly used as anchorage devices for retraction of the anterior segment. However, no scientific investigations have compared the treatment effects of MCPP with those of headgear used as active distalization appliances in adult patients, where the efficacy of the appliances could be influenced by various factors such as skeletal maturity and eruption status of the maxillary molars.
Therefore, the purpose of the present study was to evaluate the dental and skeletal effects of MCPP for total arch distalization in adult patients with Class II malocclusion and compare the findings with those of cervical pull headgear.
MATERIALS AND METHODS
The study sample comprised the lateral cephalograms of 44 patients with Class II Division 1 malocclusion; 22 (6 men, 16 women; age, 24.7 ± 7.7 years) were treated with MCPP (Jeil Medical Co., Seoul, Korea) at the Department of Orthodontics, St. Mary's Hospital, The Catholic University of Korea, while 22 were treated with cervical pull headgear (6 men, 16 women; age, 23.0 ± 7.7 years;) in a private clinic. The inclusion criteria were as follows: skeletal growth completion at the time of treatment initiation (cervical vertebral maturation stage V20), a diagnosis of Class II Division 1 malocclusion, moderate maxillary arch crowding (Little's Irregularity Index < 5 mm) with maxillary protrusion, mild mandibular arch crowding (Little's Irregularity Index < 3 mm), no tooth extraction during treatment, maxillary molar distalization that had been exclusively accomplished by either MCPP or cervical pull headgear, absence of craniofacial syndromes, and availability of high-quality lateral cephalograms and treatment records.
Table 1 shows the distribution of the severity of malocclusion with regard to the molar relationship in each group. MCPP was used to facilitate molar distalization according to the method described in previous studies.2122 The appliances were fitted on dental casts to adapt to the shape of the palatal surface, with their arms extending into the area between the first molars and second premolars. Adequate space was maintained between the arms and palatal slopes. The same operator (YAK) transferred MCPP from the cast to the oral cavity using a jig and fixed the appliance with three miniscrews measuring 8 mm in length and 2.0 mm in diameter (Jeil Medical Co.). Then, a palatal bar with two hooks extending along the gingival margins of the teeth was cemented on the right and left maxillary first molars. Immediately after placement, distalization was initiated by engaging elastics or nickel-titanium closed coil springs between the MCPP arm notches and the hooks on the palatal bar, with an approximate force of 300 g per side. The outer bows of the cervical pull headgear were adjusted slightly upward so that they passed near to the center of resistance of the maxillary first molars.
Most MCPPs and headgear were delivered with fixed appliances during the same visit. The straight wire technique with 0.022-inch-slot brackets was used for both groups, with either In-Ovation C (Dentsply GAC International, Islandia, NY, USA) or minitwin metal brackets (Ormco Co., Orange, CA, USA) depending on the patient preference. During the leveling phase, the size of the archwire was increased up to 0.018 × 0.025 or 0.019 × 0.025-inch stainless steel. Once the maxillary first molars were distalized to the intended overcorrected positions, MCPP and the cervical pull headgear were discontinued. Interarch elastics, including Class II elastics, were judiciously used, particularly during the later stages of treatment.
The study was approved by the institutional review board of the Catholic University of Korea (KC15-RISE0843). Informed consent was obtained according to the tenets of the Declaration of Helsinki. All lateral cephalograms, dental casts, facial and intraoral photographs, and treatment charts were examined in detail.
Cephalometric measurements
Lateral cephalograms obtained before the insertion of any appliance (T1) and after debonding (T2) were digitized using V-Ceph 5.5 software (Cybermed, Seoul, Korea). Two reference lines were constructed for horizontal and vertical measurements. The horizontal reference line was represented by the Frankfort horizontal (FH) plane, while the vertical reference line was defined to be perpendicular to the FH plane while passing through the pterygoid point. A total of 24 linear and angular measurements were recorded by one examiner, as shown in Figures 1 and 2. Differences between T1 and T2 findings were calculated (T2–T1) to assess the effects of treatment.
To identify systematic errors and compare measurement accuracy, 10 randomly selected cephalograms from each group were redigitized and measured at least twice on two separate occasions at an interval of 2 weeks by the same examiner. Intraexaminer reliability was evaluated using the intraclass correlation coefficient, which was found to be > 0.90 for all variables.
Statistical analysis
All statistical analyses were performed using SPSS ver. 16.0 (SPSS Inc., Chicago, IL, USA). The Kolmogorov–Smirnov method was used to confirm the normal distribution of measurements. Paired t-tests were used to evaluate skeletal, dental, and soft tissue changes from T1 to T2 in each group. Multivariate analysis of variance (MANOVA) was performed to evaluate the changes after treatment in each group and compare the treatment effects between groups. A chi-square test showed no significant differences in the distribution of malocclusion severity between the two groups (p = 0.649), while an independent samples t-test showed no significant difference in age between groups (p = 0.501). The statistical significance was initially set at 0.05. After the application of Bonferroni correction, the significance level was 0.002.
RESULTS
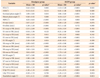
There were no significant differences in all pretreatment variables (Table 2) and all post-treatment variables except incisor mandibular plane angle (IMPA) (Table 3) between the two groups. In addition, there was no significant difference in the treatment duration between groups (MCPP, 29.9 ± 11.9 months; headgear, 24.1 ± 9.1 months; p = 0.099). Both groups demonstrated a significant decrease in the overjet, whereas only the headgear group exhibited a decrease in the overbite, which showed no significant difference between the two groups (Table 4).
The MCPP group exhibited significant changes in the position of the maxillary first molar (p < 0.001). The mean amount of distalization at the crown and root levels was 4.2 and 3.5 mm, respectively, with distal tipping of 3.9° and intrusion by 2.5 mm. Meanwhile, in the headgear group, distalization was 2.3 mm at the crown level and 0.6 mm at the root level, with distal tipping of 8.6° and extrusion by 0.4 mm. All variables were significantly different between the two groups (p < 0.001, Table 4).
The maxillary second molar also showed significant distalization of 2.4 mm at the crown level and 2.7 mm at the root level, with intrusion by 2.2 mm, in the MCPP group. However, in the headgear group, the crown was distalized by 1.9 mm, with insignificant extrusion. The amount of distalization was not significantly different between the two groups, whereas the change in the vertical position was significant (p < 0.001, Table 4).
None of the variables for the position of the maxillary or mandibular incisors showed statistically significant differences between the two groups. There was significant retraction of the maxillary central incisors in both groups (2.5 mm in the headgear group and 3.2 mm in the MCPP group, p < 0.001); however, only the MCPP group exhibited significant uprighting of the central incisors (−8.0°, p < 0.001). Interestingly, the headgear group showed a significant increase in IMPA (8.4°, p < 0.001; Table 4), which resulted in more proclined mandibular incisors compared with those in the MCPP group at the end of treatment (p < 0.001, Table 3).
There were no significant differences in the skeletal effects of treatment between the two groups. With regard to soft tissue variables, both groups showed a significant increase in the nasolabial angle and significant upper lip retraction (p < 0.001). However, none of the soft tissue variables showed a significant difference between the two groups.
DISCUSSION
In the present study, we compared the dental and skeletal effects of MCPP with those of cervical pull headgear for total arch distalization in adult patients with Class II malocclusion. MCPP resulted in a significantly greater distalization of the maxillary first molars compared with the headgear, with lesser distal tipping accompanied by intrusion.
The number of adults pursuing orthodontic treatment is on the rise because of an increase in public awareness of developing needs in the later stages of life. These patients often demand improved dentofacial appearances within a short period of time.
During insertion, MCPP enables easier access to a larger target zone and presents minimum risk of root contact compared with TADs, which are placed on the buccal surface. The superiority of MCPP over the more widely used miniscrews is probably attributed to its longer range of action, greater versatility of vector control, and the ability to sustain a heavier loading force. Furthermore, during the correction of Class II malocclusion, molar distalization without extrusion is critical to prevent clockwise rotation of the mandible. The design of MCPP enables the clinician to select the force vector and, consequently, control the vertical dimension of the molars by selecting the appropriate notches on the MCPP arms.
Park et al.15 analyzed the effects of sliding mechanics used with high-pull headgear or miniscrews for retraction of the anterior segment after extraction of the maxillary first premolars. They found decreased anchorage loss for the maxillary molars in the miniscrew group with no significant difference between groups with regard to the vertical dimension.
Later, Chen et al.19 examined the effects of headgear and miniscrew anchorage in adults with bimaxillary protrusion and concluded that miniscrew anchorage provided better control in the sagittal and vertical directions compared with the headgear.
In the present study, the mean amount of distalization at the crown level of the maxillary first molar in the MCPP group was 4.2 mm, which was significantly greater than that in the headgear group. The amount of distalization at the root level showed an even larger difference between the MCPP (3.5 mm) and headgear (0.6 mm) groups.
Before treatment, both groups showed an approximate overjet of 5 mm in the present study. In the MCPP group, the overjet was primarily corrected by retraction and retroclination of the maxillary incisors, whereas in the headgear group, a significant amount of overjet correction was achieved by proclination of the mandibular incisors while maintaining the position of the maxillary incisors. This could be attributed to the effects of leveling out the deep Curve of Spee in the mandibular arch. Interestingly, these were in agreement with the findings of Sa'aed et al.,13 who suggested that the difference could have occurred because of differences in the treatment strategy employed by two different operators.
The headgear group in the present study exhibited an increase of 4.5° in the nasolabial angle. This was in agreement with the results of Kirjavainen et al.,23 who reported a widening of 3.4° in the angle in adolescents. Our MCPP group showed a similar amount of increase in the nasolabial angle, which was 5.1°. These findings were also consistent with those of Sa'aed et al.,13 who showed a significant increase of 2.7° in the nasolabial angle after application of the palatal plate in adolescents. The difference in the amount of increase between the two studies can be attributed to the growth effects in the adolescents included in the latter study, which masked the treatment effects.
During evaluation of patient records for the headgear group, it was important to carefully screen out any evidence of poor compliance, considering that compliance is a crucial factor which dictates the success of such removable appliances. Although younger patients are reportedly more compliant,24 appropriate wear of headgear is affected by a combination of factors such as age, personality, and positive and negative motives.25 Interestingly, the adults in the headgear group in the present study displayed 2.2 mm of distalization at the crown level of the maxillary first molar, which was greater than the 1.8 mm in the adolescent group included in the study by Sa'aed et al.13 We speculate that, among more compliant orthodontic patients, the age factor becomes less dominant with regard to the effectiveness of headgear therapy.
In previous studies on the treatment effects of headgear used for adults, the appliance was worn for 10–12 hours/day.1518 This was consistent with the duration of wear in the present study (11.2 ± 2.5 hours/day). Previous studies reported that headgear anchorage in adults resulted in mesial movement of the maxillary first molar by 2.2 to 3.6 mm.1819 On the other hand, the first molars were distalized by 2.2 mm in the present study. This difference may be attributed to the difference in the treatment goal, which was to provide anchorage support in the previous studies and to distalize the maxillary dentition in the present study. However, in agreement with the findings of Park et al.,15 both groups in the present study showed significant upper lip retraction, with no significant difference in the amount of retraction between groups.
MCPP provides clinicians with three different force vector options. The clinicians may choose the one that fits best in the specific clinical situation by selecting the appropriate notches on the MCPP arms. Figure 3 shows the different force vectors that could result from engaging the different notches. The selection of the most apical position is associated with more root movement or more bodily movement26; however, it is possible that these results were affected by the shape of the palate used in the finite element model. Therefore, it may be advisable to closely monitor the relationship between applied force vectors and the clinically estimated center of resistance in the maxillary dentition for better control over the vertical dimension and the intended root movement of the molars.
Recently, Kang et al.27 reported distal tipping and extrusion of the first molar with headgear use in their finite element analysis. On the other hand, the palatal plate resulted in intrusion of the first molar accompanied by more distalization at the root level than at the crown level. These findings were in agreement with most of our findings for both groups; the amount of root movement caused by the palatal plate in our study was less than the amount of crown movement, probably because of differences in the clinical situations and finite element models.
In the present study, we used lateral cephalograms, which are two-dimensional images and have inherent disadvantages such as projection, magnification, landmark superimposition, and sensitivity to head position changes. In addition, further investigations are recommended to determine the treatment effects of MCPP, such as retraction efficiency, and associated patient perceptions in comparison with those for other anchorage units. Finally, the utilization of three-dimensional models generated from cone beam computed tomography images may be warranted to analyze the treatment effects in the rotational and horizontal planes in the future.
CONCLUSION
In conclusion, the main findings of our study were as follows.
Distalization of the maxillary first molar in adult patients with Class II malocclusion were significantly greater with MCPP than with cervical pull headgear.
Maxillary first molar intrusion was observed in the MCPP group, whereas slight extrusion as observed in the headgear group.
Both groups showed significant upper lip retraction and a significant increase in the nasolabial angle.
These findings suggest that MCPP is an effective treatment modality with improved root control for maxillary molar or total maxillary arch distalization.





 XML Download
XML Download