This article has been
cited by other articles in ScienceCentral.
Abstract
Objective
Teeth discoloration is a rare orthodontic complication. The aim of this study was to report the clinical progression of discoloration during orthodontic treatment.
Methods
Discolored teeth, detected during orthodontic treatment between January 2003 and December 2012 by a single dentist using similar techniques and appliances, were analyzed.
Results
The total number of teeth that showed discoloration was 28. Progression of discoloration was evaluated in only 24 teeth that were observed without any treatment. During the observation period, the discoloration “improved” in 8 of the 24 teeth (33.3%) and was “maintained” in 16 (66.6%). The electric pulp test performed at the time of initial detection of discoloration showed 14.3% positivity, which improved to 21.4% at the final follow-up. None of the initial and final follow-up radiographic findings showed any abnormalities.
Conclusions
When teeth discoloration is detected during orthodontic treatment, observation as an initial management is recommended over immediate treatments.
Keywords: Esthetics, Perception, Diagnosis and treatment planning
INTRODUCTION
During orthodontic treatment, the color of teeth may darken to gray or brown as a sign of discoloration, necrosis, or devitalization of the pulp. Tooth discoloration is a rare phenomenon, however it may come to patients as a disturbance which may disrupt the doctor-patient relationship.
Previous case reports have documented pulp necrosis or devitalization,
12 and animal studies have been conducted on the reduction of pulpal blood flow (PBF) caused by orthodontic force.
34 Some human studies have also measured PBF by using laser Doppler flowmeters,
56 and most of these studies showed an initial reduction in PBF, which recovered after the removal of the orthodontic force. In another report, Sano et al.
7 applied continuous intrusive force (0.5 N for 6 days) on the maxillary anterior teeth of 13 patients and found that PBF significantly decreased only while the force was applied, and was restored when the force was removed.
In 2014, González et al.
8 reported the case of a 48-year-old man whose maxillary central incisor became discolored 5 weeks after the application of orthodontic force. The patient did not receive active intervention, such as endodontic treatment. After 10 weeks of observation, the gray discoloration disappeared and the tooth showed a normal response to clinical tests (cold, percussion, and plain radiographic examinations). This was referred to as transient apical breakdown (TAB). These signs of TAB usually return to normal without serious complications, and only periodic follow-ups are recommended.
910
However, previous studies have focused either on animal experiments or, in the case of humans, on a specific tooth of a specific patient over a short time period. No long-term clinical study has been performed in humans. Cho et al.
11 even stated there were only anecdotal reports and no clinical data regarding the incidence of pulpal necrosis after orthodontic therapy.
Therefore, the aim of this study was to report on the clinical progression of discolored teeth.
MATERIALS AND METHODS
Data were collected from patients in whom discolored teeth were discovered during orthodontic treatment between January 2003 and December 2012. They were treated by a single dentist who used similar techniques and appliances. The teeth of the patients who had received orthognathic surgery or experienced any trauma or pathological problems were excluded.
Assessment of discoloration was performed under the following conditions:
If the discoloration was detected under dental light, natural light, or interior lighting, intraoral photographs were acquired. These photographs were then compared to previous photographs and a first panel (one dentist, the patient, and two dental hygienists) confirmed the discoloration.
Comparisons of intraoral photographs were conducted again 2 weeks later by a second panel (the same dentist from the first panel and two other dental hygienists), and if the discoloration was still confirmed, then those teeth were selected for analysis.
The first panel excluding the patient evaluated the color change by comparing the initial intraoral photographs to the follow-up photographs. Intraoral photographs were imported to a PowerPoint (Microsoft, Redmond, WA, USA) slide with a black background. If the tooth regained some or all of its original color, then the condition was defined as “improved” (Figure 1), and if the color remained, then the condition was defined as “maintained” (Figure 2). If the color had darkened, this was defined as “worsened.” Two weeks later, the discoloration was re-evaluated by the second panel.
Intraoral photographs were acquired via a single camera model (D50, AF-S DX ED18-70; Nikon, Tokyo, Japan).
When discoloration was discovered, plain radiographs were acquired, and an electric pulp test (EPT) was performed.
RESULTS
Discoloration was discovered in 28 teeth (
Table 1). These included seven maxillary central incisors, one maxillary lateral incisor, 11 maxillary canines, five mandibular incisors, one mandibular canine, and three mandibular premolars. There was no discoloration in the molars.
One patient remembered experiencing a symptom of slight sensitivity when the discoloration was discovered (
Table 2). Out of the 28 teeth, we evaluated the color change in 24 teeth that were only observed without any treatment.
Among the 24 observed teeth that received no treatment, the discoloration improved in eight (33.3%), was maintained in 16 (66.6%), and worsened in none. The EPT results at the point of initial detection (EPT_ini) were positive in four teeth (14.3%). The EPT results at the final follow-up (EPT_fu) were positive in six teeth (25.0%). In some cases, changes were observed in the EPT_ini and EPT_fu. Three teeth had a negative EPT_ini, which changed to a positive EPT_fu, and one tooth had a positive EPT_ini, which changed to a negative EPT_fu. None of the 28 teeth showed any abnormalities on either initial or follow-up radiography (X_ini and X_fu, respectively) (
Table 2).
DISCUSSION
Compared to other orthodontic complications such as root resorption, gingival recession, white spot lesions, or root dehiscence, tooth discoloration rarely occurs. However, any orthodontist may encounter this complication.
Of the 28 discolored teeth, the number of maxillary canines and maxillary central incisors were the highest at 11 and 7, respectively. We suspected this was because both these teeth have single long roots, which may cause PBF to be more easily disturbed. No discoloration occurred in the molars, possibly because they have multiple roots, which result in fewer disturbances in PBF. Discoloration was also more frequent in the maxillary teeth than in the mandibular teeth, possibly due to the overjet relationship which may increase susceptibility to trauma in the maxillary teeth. Mild discoloration may be overlooked without being detected, as in some cases, the discoloration may even disappear without any treatment. Thus, discoloration may be detected at a higher rate when teeth are examined under persistent clinical scrutiny.
One of the limitations of this study was the establishment of a scientific and objective standard on the definition of discoloration. Instruments such as spectroradiometers, tristimulus colorimeters, and spectrophotometers are used to scientifically and objectively measure color change. However, the most realistic method, and the best currently available, is comparing tooth color by using intraoral photographs. Huang et al.
12 performed an objective evaluation of color change for white spot lesions, in which four panels were created to evaluate discoloration under as much identical circumstances as possible. Our research was conducted in close reference to their study.
Another limitation of this study was the lack of data regarding the incidence of discoloration. More important than the number of patients with tooth discoloration is the incidence of discoloration in each tooth, which must be calculated only on the basis of the teeth on which orthodontic force was applied. There could also be partial orthodontics, mixed dentition (including deciduous teeth), and additional brackets bonded after the start of treatment. Monitoring all these teeth for 10 years is very hard work and virtually impossible.
When discoloration occurs, can pulp vitality be considered lost? Pulp vitality must be evaluated on the basis of a holistic evaluation of history taking, clinical examinations including pulp tests, and plain radiographic findings. At the initial detection of discoloration, the EPT showed a negative response in 85.7% of the discolored teeth, while symptoms such as pain, sensitivity, or adjacent tissue swelling were mostly absent except for mild sensitivity in one tooth. Moreover, all the plain radiographic findings were normal. At the final follow-up, none of the plain radiographic findings revealed any abnormalities, and there were no abnormal symptoms. In the EPT, the three teeth that had a negative response at initial detection later showed a positive response, and the opposite trend was observed in one case (positive to negative response). Orthodontic tooth movement can lead to biological reactions in the periodontal ligament and dental pulp, and one of these is TAB.
8910 In TAB, initially, there will be some radiographic widening of the periodontal ligament and a small area of apical radiolucency, which can result in discoloration. However, these changes are transitional, and injured tissues usually undergo a spontaneous process of repair with no permanent damage to the pulp. The time required for this to occur can vary and may take as long as 1 year after the removal of the cause. If this phenomenon is misdiagnosed, however, the doctor may proceed to endodontic or prosthetic treatment. In this study, we had excluded four cases in which such treatment had been initially performed. Once a better understanding of this phenomenon was gained, only observation was performed. Discoloration is a change in tooth color due to hyperemia of the pulp or hemoglobin accumulation in the pulp tissue. Discoloration is a reversible state, whereas pulp necrosis is not. The term discoloration is used to represent a symptom, not a pathologic disease. Considering all of the above factors in this study, we could suggest that discoloration does not always indicate pulp necrosis or devitalization.
CONCLUSION
On the basis of the findings of this study, the following suggestions can be made:
When discoloration occurs, first reduce or remove the orthodontic force to enable the recovery of PBF.
Thoroughly observe the color change and defer irreversible treatment.
If discoloration does not improve even after sufficient observation, perform treatments such as endodontic or prosthetic treatment, or bleaching.
Inform the patient that discoloration does not always indicate devitalization or pulp necrosis.
The term “discoloration” is recommended over “pulp necrosis” or “devitalization.”
Figures and Tables
 | Figure 1An example of “improved” discoloration (maxillary right central incisor). A, Start of treatment. B, Initial discovery of discoloration. C, Debonding. D, 71 months after the initial discovery of discoloration.
|
 | Figure 2An example of “maintained” discoloration (mandibular right second premolar). A, Start of treatment. B, Initial discovery of discoloration. C, Debonding. D, 45 months after the initial discovery of discoloration.
|
Table 1
Mean and proportion of data (n = 28)


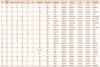
Table 2
Summary of total data


 PDF
PDF ePub
ePub Citation
Citation Print
Print


 XML Download
XML Download