

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Congenitally missing teeth is a common dental anomaly and the most frequently missing teeth are the mandibular second premolars.123 Patients with hypodontia are generally presented with several other dental anomalies such as retained deciduous teeth, impactions, transpositions, and peg-shaped lateral incisors.4567 These cases are most often referred for an interdisciplinary approach with orthodontic and restorative treatment.
Patients with multiple missing teeth are usually reluctant for further extractions of deciduous teeth in good condition, even though the long-term prognosis is uncertain. If an adolescent patient has a good profile with minimal crowding, most clinicians would agree to keep the retained deciduous tooth until natural exfoliation occurs. However, if the retained tooth was a mandibular deciduous second molar, the mesiodistal dimensions are larger than a permanent premolar which would need reshaping into the size of a permanent premolar or could be left in situ with less than ideal but functional occlusion depending on the clinician's judgment and patient's disposition towards treatment.8
Here, we present a 5-year follow up of an adolescent patient with congenitally missing mandibular second premolars and maxillary lateral incisor. This patient also had retained deciduous mandibular second molars and maxillary canines, impactions, transpositions and a peg shaped lateral incisor. This case report successfully demonstrates that maintaining retained deciduous teeth in situ can be a viable treatment option with good long term results in complex orthodontic cases involving missing permanent teeth and other associated dental anomalies.
DIAGNOSIS AND ETIOLOGY
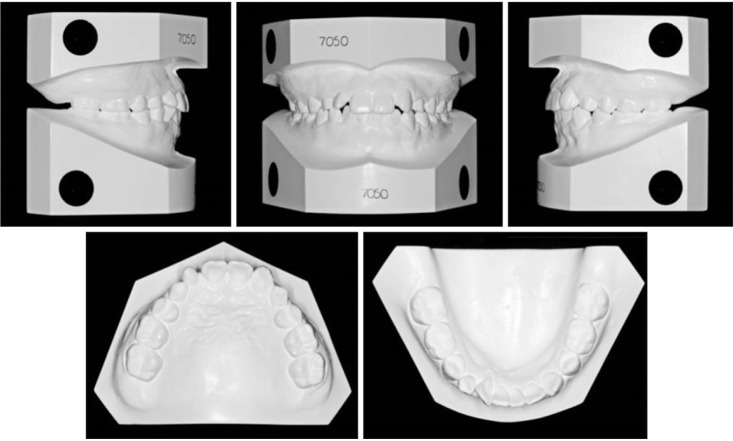
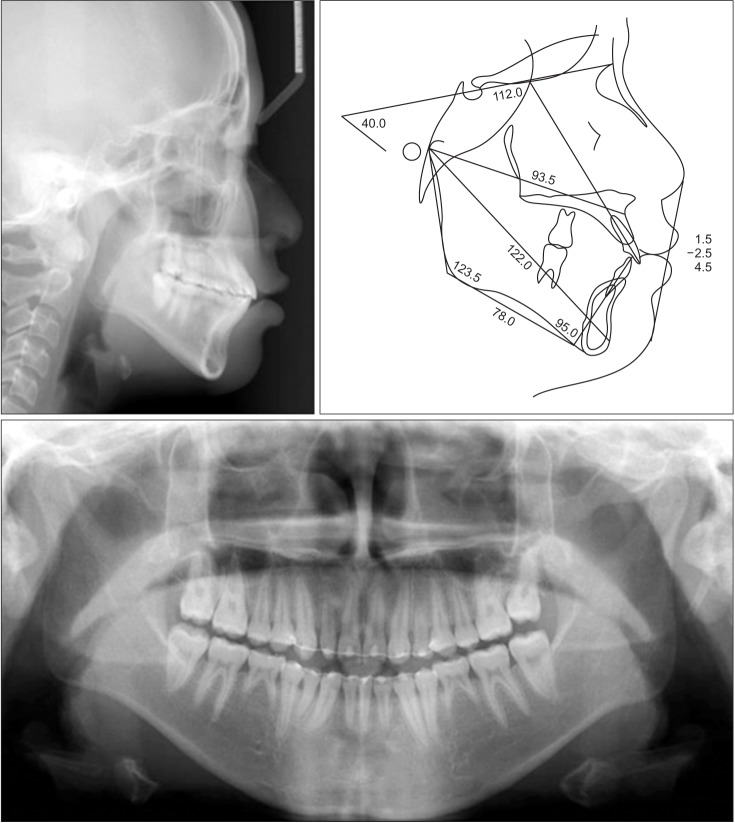
A 15-year-old boy visited the Department of Orthodontics in Gangnam Severance Dental Hospital (Seoul, Korea) in 2006 with a chief complaint of missing mandibular second premolars and a maxillary lateral incisor and impaction of canines (Figures 1, 2, 3). Besides
atopic dermatitis, the patient was in good health and did not have any contraindications to dental treatment. The patient did not have any history of trauma to the face or teeth, but a family member had congenitally missing mandibular second premolars as well.
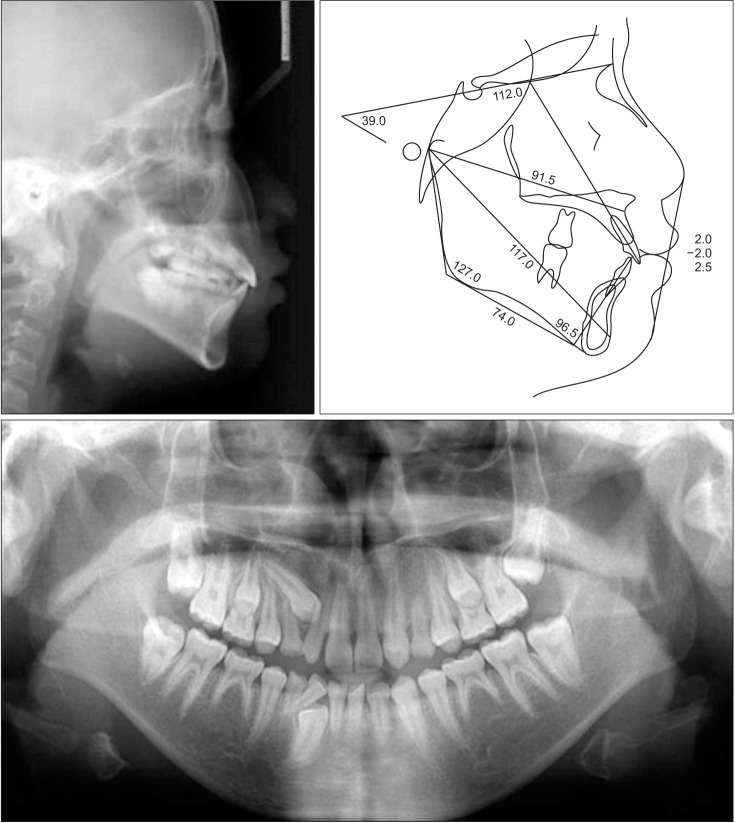
A pretreatment panoramic radiograph showed that teeth 22, 35, and 45 (Federation Dentaire Internationale numbers) were congenitally missing while teeth 75 and 85 were retained (Figure 3). Tooth 23 had ectopically erupted into the space of the missing tooth 22 and deciduous tooth 63 was retained with clinically acceptable root length. The retained 75 and 85 were not submerged in relation to their adjacent teeth. The crown of impacted tooth 13 was positioned between the roots of teeth 12 and 53, with an overlap of less than half the root width of the lateral incisor which was a favorable position for forced eruption. Eruption of tooth 27 was obstructed by the position of tooth 26 which resulted in a mesially directed crown impaction. The impacted tooth 43 was in a transposed position mesial to tooth 42 which showed lingual gingival recession (Figures 1 and 2). Tooth 12 displayed a peg shaped clinical crown.
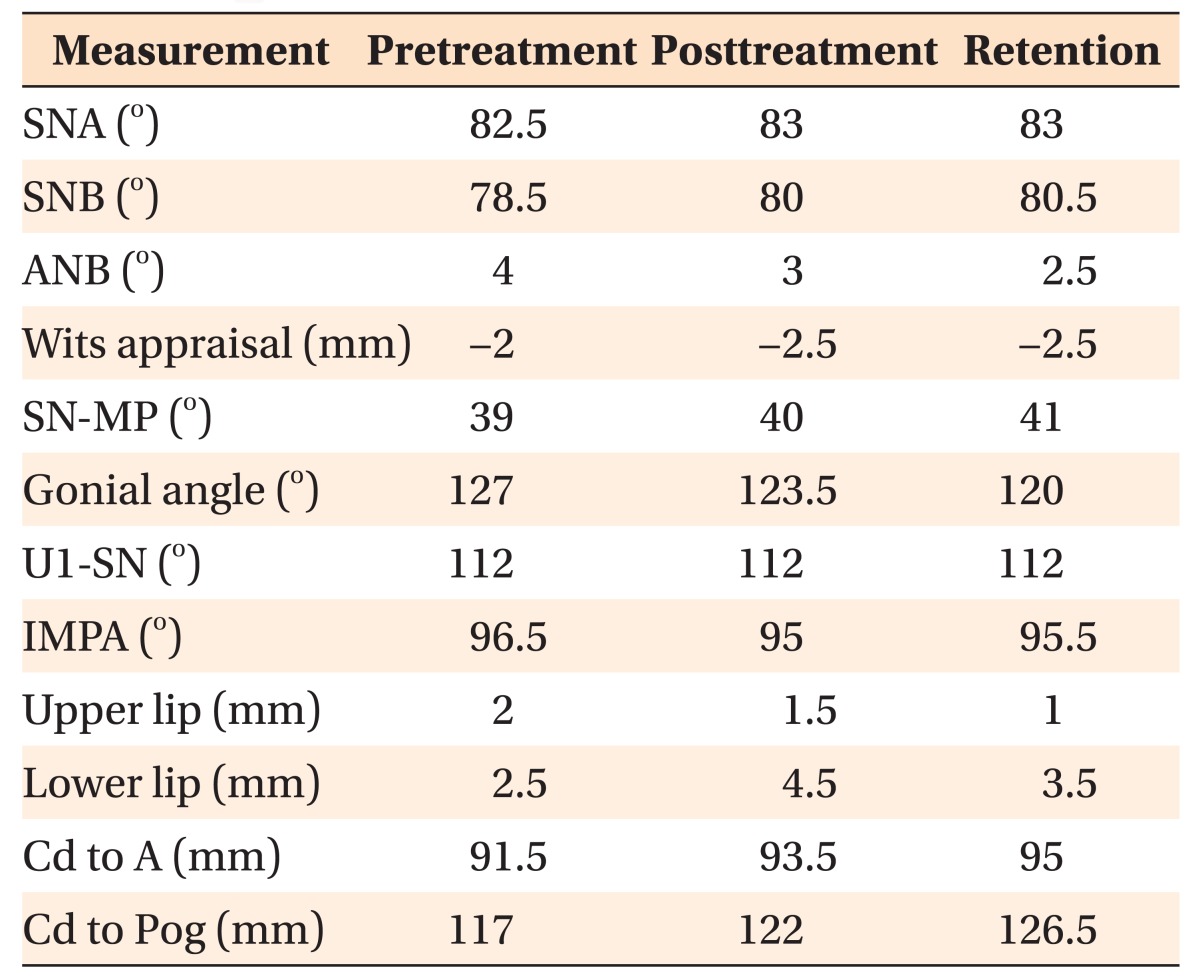
Cephalometric analyses showed a skeletal Class I relationship with an A point-nasion- B point (ANB) angle of 4.0° and a normodivergent facial profile (Table 1). The maxillary incisors were proclined (angle between upper incisor and sella-nasion line [U1 to SN], 112°) and the mandibular incisors showed a normal inclination to the mandibular plane (IMPA, 96.5°; Figure 3). The dental midlines were aligned and the molars were in an Angle Class II relationship due to retained teeth 75 and 85 (Figures 1 and 2). The patient had a good facial profile and no asymmetries were noted. The patient's skeletal age was assessed as stage 7 according to skeletal maturity index (SMI) of Fishman9 which indicated a considerable amount of growth was still remaining.
Upon these findings, the patient was diagnosed as skeletal Class I malocclusion with congenitally missing mandibular second premolars and a maxillary lateral incisor, with retained deciduous teeth, impactions and transpositions.
TREATMENT OBJECTIVES
The treatment objectives for this patient were to establish functional occlusion by guided eruption of the impacted teeth, to preserve the alveolar bone for the congenitally missing teeth area until completion of growth, and to maintain good soft tissue balance.
TREATMENT ALTERNATIVES
All treatment plans included the following treatment. Retained deciduous teeth 53 and 83 would be extracted to facilitate eruption of teeth 13 and 43. Tooth 43 was left to erupt into its transposed position because it was located mesial to tooth 42 at root level. Tooth 27 would be monitored for spontaneous eruption.
The first option for deciduous teeth 75 and 85 was to maintain the teeth in situ. This was possible because the roots of the deciduous molars were not extensively resorbed, the teeth were clinically stable without mobility and showed favorable vertical position in the occlusal plane. Although the molar relationship would remain Angle Class II, the patient would have functional occlusion. The second option was to reduce the width of teeth 75 and 85 to the size of a permanent second premolar. This option would maintain the buccolingual bone for an eventual implant. However, extensive reshaping of the deciduous molars would be limited because of root divergence.
Treatment options for the missing tooth 22 were to maintain tooth 63 and reshape tooth 23 into an incisor, or to extract tooth 63 and distally move tooth 23 to create space for prosthetic restoration. If the first option was selected, the gingival contours and color of tooth 23 would not fully match those of the contralateral incisor. Also, if tooth 63 were to fail in the long term, the space of tooth 23 would have to be restored. As for the second option, the lateral incisor space would need a temporary restoration and alveolar bone level should be monitored.
The patient was informed that, although the retained deciduous teeth appeared clinically stable, this did not guarantee a good prognosis for long-term survival. Decision for a final treatment plan was based on the patient's interest for the most conservative treatment that required minimal prosthetic treatment following orthodontic treatment. The family opted to maintain the deciduous mandibular second molars and maxillary canine.
Accordingly, the final treatment plan consisted of extraction of teeth 53 and 83, surgical opening for tooth 13 and eruption guidance of teeth 13, 43 and 27. Deciduous teeth 63, 75, 85 would be left in situ and incorporated into final occlusion. Tooth 23 would be reshaped into a lateral incisor during alignment and the peg lateral tooth 12 would be restored by prosthetic treatment after orthodontic treatment. Periodic evaluation of retained deciduous teeth 63, 75, 85 would be scheduled after orthodontic treatment.
TREATMENT PROGRESS
Deciduous teeth 53 and 83 were extracted and a mucoperiosteal flap was raised along the gingival margin for surgical opening of tooth 13. A sufficient portion of the tooth 13 was exposed for resin bonding of a button. The mucoperiosteal flap was repositioned, leaving a twisted wire for orthodontic traction.
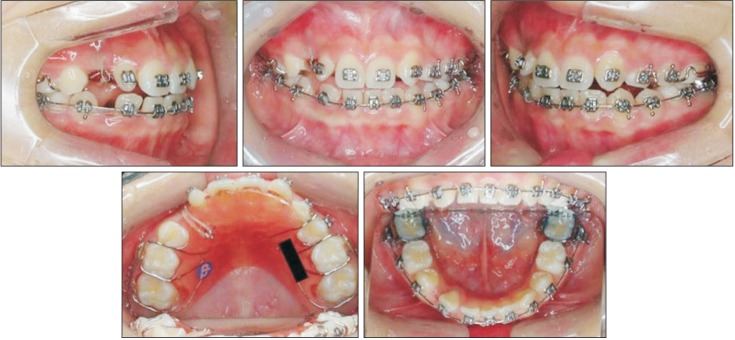
Roth prescription brackets (0.018-inch; Tomy, Tokyo, Japan) were bonded and initial forces were applied with 0.016-inch nickel-titanium (Ni-Ti) wires. A maxillary removable appliance was used with elastics for guided eruption of tooth 13 until a rigid wire was inserted in the maxillary arch (Figure 4). After 3 months, the archwires were changed to 0.016 × 0.022-inch stainless steel. An elastomeric chain was extended from the twisted wire of tooth 13 to a hook attached to the maxillary archwire for continuous traction forces. In the mandibular arch, distal force was applied to tooth 42 using an open coil spring to create space for spontaneous eruption of tooth 43 into the transposed position mesial to tooth 42.
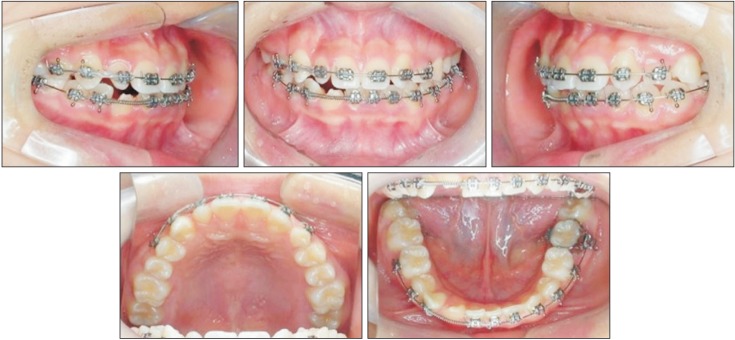
Teeth 15 and 25 erupted into the arch after natural exfoliation of the deciduous teeth 55 and 65 which occurred about 6 months into treatment and brackets were bonded for alignment. Eruption of impacted tooth 27 was facilitated by the mesial drift of tooth 26 after exfoliation of the deciduous tooth 65. Eruption of tooth 13 occurred after 9 months of guided eruption (Figure 5), and a 0.016-inch Ni-Ti overlay wire was used for alignment. After 16 months, tooth 43 erupted naturally in the space created between teeth 41 and 42 (Figure 6). After additional leveling and alignment, occlusal seating and detailing were accomplished. Teeth 23 and 43 were slightly extruded to match the gingival contour of the adjacent teeth and reshaped into incisors.
The appliances were removed after a total treatment time of 32 months and lingual fixed retainers were bonded (Figures 7, 8, 9). Prosthetic treatment on tooth 12 was postponed until growth completion upon patient's request. Additional retention was provided by circumferential retainers. The patient returned periodically over the next 5 years for follow-up examinations.
RESULTS
Impacted teeth 13 and 43 were brought into the arch. The retained primary teeth 63, 75 and 85 remained clinically stable with little changes in root resorption after 32 months of treatment. Teeth 23 and 43 were reshaped into an incisor without further prosthetic treatment. Although the gingival margins of the maxillary teeth were not ideal due to the transposed tooth 23 and retained primary tooth 63, the patient had a relatively low smile line which was a positive influence to esthetics. Lingual gingival recession of tooth 42 was resolved by relief of crowding and orthodontic alignment. Impacted tooth 27 was left to erupt naturally into the arch and showed acceptable occlusion (Figures 7, 8, 9).
Treatment was completed with a Class II molar relationship due to retained 75 and 85. Nevertheless, the palatal cusps of the maxillary premolars were in good functional occlusion with the deciduous mandibular second molars. Although the overjet and overbite relationships were ideal, the mandible had dental midline deviation of 1.5 mm to the left, which was a result of slight facial asymmetry that occurred with growth and transposition of teeth 42 and 43. Incisal and lateral guidance were present despite the fact that teeth 63 and 42 were in place of a permanent canine (Figures 7 and 8).
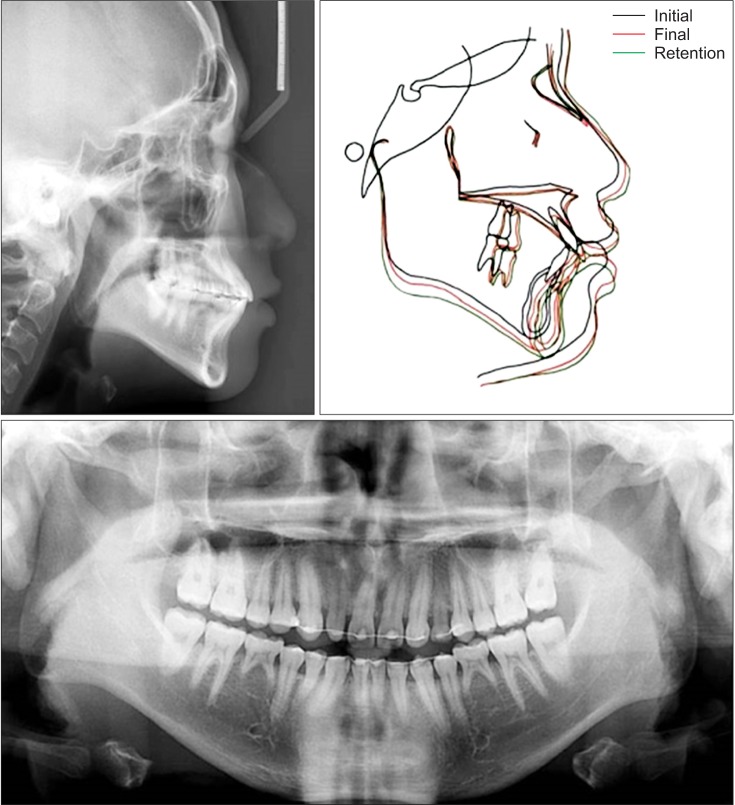
The final panoramic radiograph showed good root alignment (Figure 9). Slight root resorption was noted in the retained deciduous teeth, which were monitored throughout the follow-up period. Cephalometric analysis showed continuous Class I normodivergent growth pattern, with an increase in the maxillary and mandibular lengths due to craniofacial growth during the 32 months of treatment. Maxillary and mandibular incisor inclinations were maintained and lip positions were acceptable showing good patient profile (Figure 9 and Table 1).
Panoramic radiographs taken at the 5 year retention visit show deciduous teeth 75 and 85 still in functional occlusion and clinically stable with little root resorption (Figure 12). The mesial inclination of tooth 27 had decreased with continuous eruption into occlusion. The transposed tooth 42 remained functional as a mandibular canine and does not show clinical or radiographic signs of trauma from lateral guidance. In a similar note, primary tooth 63 maintains its favorable prognosis in place of a permanent canine at the 5 year retention visit. However, a diastema between teeth 11 and 21 has occurred despite the bonded fixed retainer. The spaces mesial and distal to the unrestored peg lateralis tooth 12 has somewhat increased as well (Figures 10, 11, 12). The patient's skeletal age was assessed as SMI stage 9 at treatment completion and stage 10 at the 5-year visit. Superimposition of lateral cephalograms obtained before, after, and 5 years after treatment showed that a skeletal Class I growth pattern was maintained throughout the pubertal period (Figure 12).
DISCUSSION
It is difficult to establish a treatment plan for an adolescent patient with missing permanent teeth and several other dental anomalies, considering that treatment cannot be finalized until growth completion. Patients with several missing permanent teeth may be inclined towards a decision of keeping the retained deciduous teeth. The patient presented in this report had missing mandibular second premolars and a maxillary lateral incisor with several other dental anomalies that further complicated orthodontic treatment and its stable retention.
Orthodontic treatment may be applied to retained deciduous teeth that are included in the final occlusion. Orthodontic forces promote stress on periodontal ligaments, followed by accumulation of mediators and bone resorption on periodontal surface of the alveolar bone in permanent or deciduous teeth alike.10 As all roots are at a risk for some resorption during orthodontic traction, there has been no direct comparison of orthodontic effects on root resorption between permanent and deciduous teeth.11 In the present case, the retained deciduous mandibular second molars and maxillary canine showed little root resorption even after orthodontic treatment.
With regard to the long-term prognosis of retained deciduous teeth, it has been reported that intact deciduous second molars with good crowns, roots, and supporting alveolar bone that survive into adulthood continue to function for many years.1112131415 A previous study stated that retained deciduous molars with agenesis of the premolars had good prognosis after age 20 years.16 A study by Hvaring et al.17 suggested infraocclusion and root resorption as critical factors for predicting the prognosis of retained deciduous teeth. In this case, the deciduous maxillary canine and mandibular second molars did not show infraocclusion, and the amount of root resorption was minimal. The patient was reluctant to have further extractions, and a decision was made to preserve the deciduous teeth in situ as long as possible. Posterior occlusion was finished in sound group function as a mandibular lateral incisor and a maxillary deciduous canine were aligned into the space of a permanent canine. Appropriate occlusal function of the deciduous teeth may prevent atrophic changes in the periodontal ligament and alveolar bone.18 In addition, even distribution of occlusal forces into group function could have avoided excessive stress concentration on the retained deciduous teeth, resulting in long-term stability. At the 5 year visit, the patient was over 20 years old, and the retained deciduous mandibular second molars and maxillary canine still showed clinical stability and little progression of resorption. Suffice it to say that the treatment plan to conserve the deciduous teeth has worked well for the patient.
The present case exhibited several impacted teeth, each of which was treated in a different manner. A closed eruption technique was used for impacted tooth 13 because the crown was positioned above the mucogingival junction and in alveolus.1920 The canine erupted into the dental arch 9 months after guided eruption. On the contrary, impacted tooth 27 was observed for spontaneous eruption, because tooth 26 was expected to drift mesially after exfoliation of tooth 65. As anticipated, tooth 27 erupted into functional occlusion without orthodontic forces despite the fact that a mesial inclination still remains during the follow up visits.
This case was finished by allowing the ectopic eruption of an impacted mandibular canine between the mandibular central and lateral incisor. Mandibular tooth transpositions are less frequently observed and the prevalence rate for transpositions of the mandibular lateral and canine is about 0.03%.2122 In the present case, both crowns and entire roots of the involved teeth were found parallel in their transposed positions which indicated a complete transposition.23 Considering the integrity of the dental arch and periodontal condition of tooth 42 which showed lingual gingival recession, correction of the transposition was not recommended. Therefore, a decision was made to move tooth 42 distally into the space of the canine and tooth 43 was left to erupt into its transposed position with favorable periodontal results. The gingival and alveolar bone levels were well maintained in the transposed area as shown in the panoramic radiograph and intraoral photos taken at the 5 year retention visit.
Esthetic requirements for canines replacing incisors should be considered and the limitations should be discussed with the patient. Esthetics can be compromised if the canine is dark in shade and a considerable size reduction is needed which could display underlying dentine.2425 The patient's smile should be considered as well because the gingival margins of the incisor and canine teeth are relatively different and subsequent gingival recontouring could be necessary in high smile line cases. Teeth 23 and 43 were similar in width to an incisor which aided in a small amount of tooth reshaping. However, the canines were relatively dark in shade, which was not a concern to the patient. Even though the gingival margin of tooth 13 was slightly apical to the adjacent teeth, gingival recontouring was not recommended due to a low smile line. The peg lateral tooth 12 was scheduled for a veneer after debonding of fixed orthodontic appliance. However, the patient decided to postpone further prosthetic treatment.
CONCLUSION
Patients with tooth agenesis and retained deciduous teeth usually exhibit other dental anomalies such as impactions, transpositions, and malformations of teeth. These cases are often found in growing patients and may pose a challenge to establishing a final treatment plan. However, early diagnosis, timely treatment, and an interdisciplinary approach involving orthodontic and restorative treatment may offer more treatment options, which can increase the quality of treatment. This case demonstrated that retained deciduous teeth with good prognosis can be incorporated into final occlusion and may display favorable long term clinical results.






 XML Download
XML Download