

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The smile is one of the most essential human facial expressions1 that enhances the reward value of an attractive face.2 Goldstein3 stated that the smile ranks second only to the eyes as the most fundamental feature affecting facial attractiveness. An attractive smile helps win elections and sell products for companies.4 Ackerman et al.5 have suggested that not all successfully treated orthodontic patients with excellent occlusal relationships and exemplary plaster models have acceptable esthetics when smiling. In traditional orthodontic treatment, orthodontists focus on teeth alignment, occlusal relationship, and function. Patients, however, are concerned about their facial esthetics, particularly smile esthetics. Most patients seek orthodontic treatment for esthetic purposes. Consequently, it is crucial for an orthodontist to be able to assess smile esthetics in a patient.4
Various factors contribute to smile esthetics. In 1958, Frush and Fisher6 introduced this concept in prosthodontic dentistry. Regarding orthodontic treatment, Hulsey7 was the first to quantify the lip-teeth relationship during smiling. He measured the smile line ratio, smile symmetry ratio, buccal corridor ratio, upper lip height, and upper lip curvature and concluded that a smile line ratio close to 1.00 produced an attractive smile. Sarver4 defined the ideal smile arc as the curvature of the incisal edges of the maxillary incisors and canines parallel to the curvature of the lower lip upon smiling.
Numerous studies have been published regarding smile esthetics. Some investigations have applied quantitated or quantified measurements to analyze the lip-teeth relationship.891011 Some other studies have assessed smiles by employing subjective esthetic evaluation, wherein evaluators were asked to rank the attractiveness of the participants' smiles.912131415
So far, there have been no studies in the field of orthodontics that investigated the effect of smile esthetics on the different kinds of malocclusion for clinical reference. Therefore, in this study, our aim was to quantitatively assess the relationship of smile esthetic variables with various types of anterior overjet (OJ) malocclusion, and identify the cephalometric factors affecting smile measurements in different types of anterior OJ malocclusion. The null hypothesis of our study was that smile characteristics differ between different types of anterior OJ malocclusion.
MATERIALS AND METHODS
Ethical approval for this retrospective study was obtained from the Institutional Review Board of Taipei Medical University (approval number: 201503035). The participants were patients who were treated with retention at the orthodontic department of Taipei Medical University Hospital from 2011 to 2013.
To be included in this study, patients had to satisfy the following criteria: (1) the patient's age at the time of treatment initiation was > 18 years; (2) orthodontic treatment had been completed; (3) an intact set of diagnostic pretreatment and post-treatment records was available, including study models, panoramic radiographs, and intra- and extraoral photograph series; and (4) pretreatment and post-treatment posed smile photographs had been taken with the patient's eyes open and a natural-looking posed smile.
The participants were divided into the following 3 groups according to their OJ: Group J1 (OJ, 0–4 mm), Group J2 (OJ, > 4 mm), and Group J3 (OJ, < 0 mm). With a sample size of 90 (i.e., 30 patients per group), a one-way analysis of variance would have 97% power at a significance level of 0.050 to detect a difference in means of arc ratio characterized by a variance of means of 0.019, assuming the common standard deviation to be 0.30.
Cephalometric analysis
All pretreatment lateral cephalograms were traced using Viewbox software® (version 3.1.1.14; dHAL, Kifissia, Greece) by one examiner (P.C.C). Figure 1 illustrates the cephalometric measurements. To verify the reliability of the measurements, 30 lateral cephalograms (10 from each group) were randomly selected from previously evaluated radiographs, and were retraced and redigitized by the same examiner after 3 or 4 weeks. Method errors were calculated using the Dahlberg's formula.16
Smile analysis
A well-trained photographic assistant who is responsible for taking all photographs in our department obtained the pretreatment photographs using a digital camera (Av mode with F4.5, ISO 1600 and flash of Canon EOS 550D, Melville, NY, USA). The distance between the patient and the camera was maintained at 150 cm in all cases, and a camera tripod was used. According to the standard operating procedure in our department, the photographic assistant instructed patients to say “seven” or “cheese” while the photograph was being clicked. The patients practiced thrice before the photographs were taken, and smiled in a natural, relaxed manner with a natural head position.
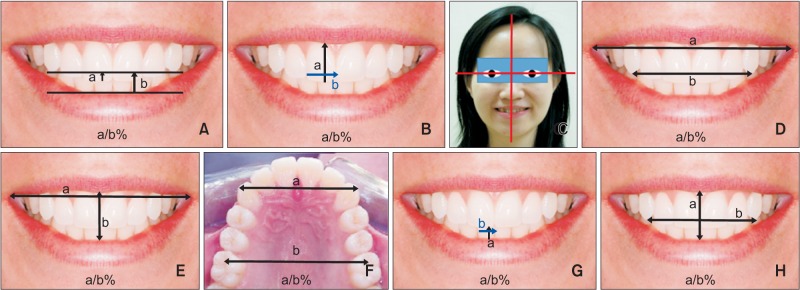
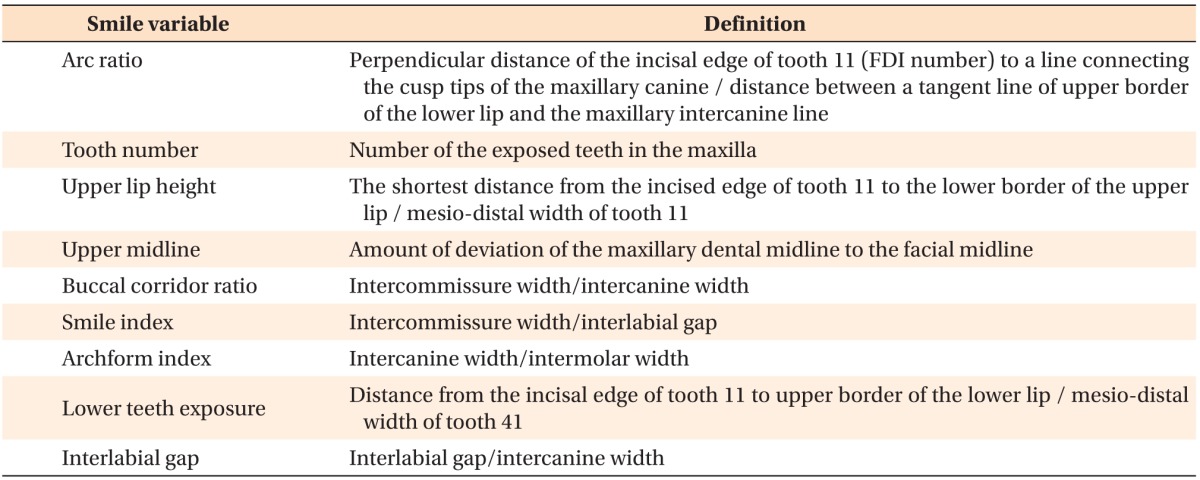
The smile variables have been evaluated separately in previous studies4567; we used these values as reference values. Because the absolute values of these parameters can vary depending on the patient's built, photo variation, and other factors, we modified the smile variables as proportions (a/b%) to minimize errors and to increase reliability. Nine smile variables (Figure 2) were measured using the linear measurement digitizer tool in Adobe Photoshop software (CS; Adobe Systems, Inc., San Jose, CA, USA) to the nearest 0.01 mm by one investigator (P.C.C.). All smile variables were evaluated as a ratio except for tooth number and the upper midline (Table 1). The reproducibility of the evaluation process was evaluated by the same investigator, who remeasured 30 randomly selected images (10 from each group) after a 1-month interval using a Student's t-test for paired samples. The absence of a significant difference (p < 0.05) between the two sets of measurements indicated agreement between them.
Statistical analysis
Statistical analyses were performed using SPSS software (version 17.0; IBM Corp., Armonk, NY, USA). Analysis of variance (ANOVA) was used to compare the pretreatment cephalometric variables and smile esthetic variables between the 3 groups. A post hoc test was performed using the Student-Newman-Keuls method. The level of significance was set at p < 0.05.
Multiple linear regression analysis was performed to identify the cephalometric factors affecting smile measurements in different types of malocclusion by using the smile variables as the dependent variables and the cephalometric measurements as the independent variables.
RESULTS
A total of 106 patients (74 women and 32 men; mean age, 25.42 ± 5.1 years; age range, 19 to 48 years) who fulfilled the inclusion criteria were included in this study. The composition of the three groups was as follows: Group J1, n = 30 (6 men and 24 women; mean age, 24.03 ± 4.5 years); Group J2, n = 34 (11 men and 23 women; mean age, 26.14 ± 6.0 years); and Group J3, n = 42 (15 men and 27 women; mean age, 25.81 ± 4.43 years).
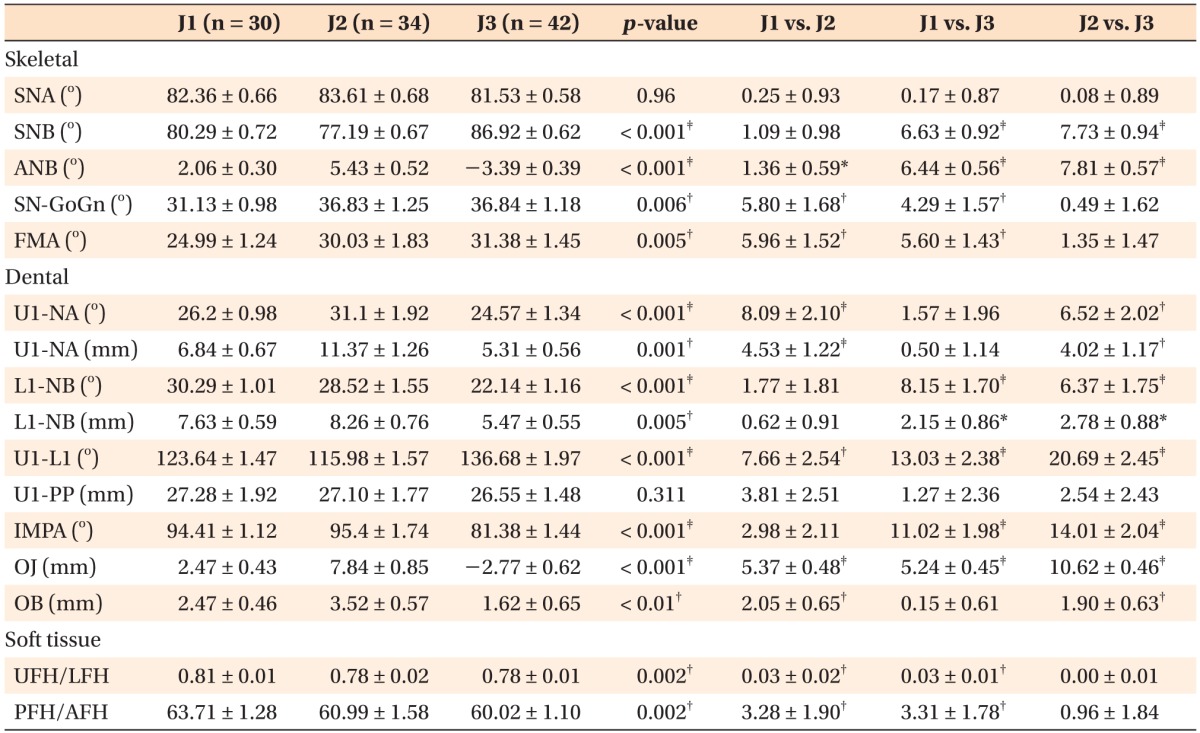
Table 2 presents the descriptive statistics of the cephalometric measurements and statistical comparisons between the three groups. The ANOVA results revealed that sella–nasion–B (SNB), A point–nasion–B (ANB), U1-NA (°), U1-NA (mm), L1-NB (°), L1-NB (mm), U1-L1, OJ, overbite (OB), incisor mandibular plane angle (IMPA), upper facial height (UFH), and lower facial height (LFH) differed significantly among the groups before orthodontic treatment. The errors for angular measurements varied from 0.23° to 1.15°, and the errors for linear measurements ranged from 0.21 to 0.98 mm.
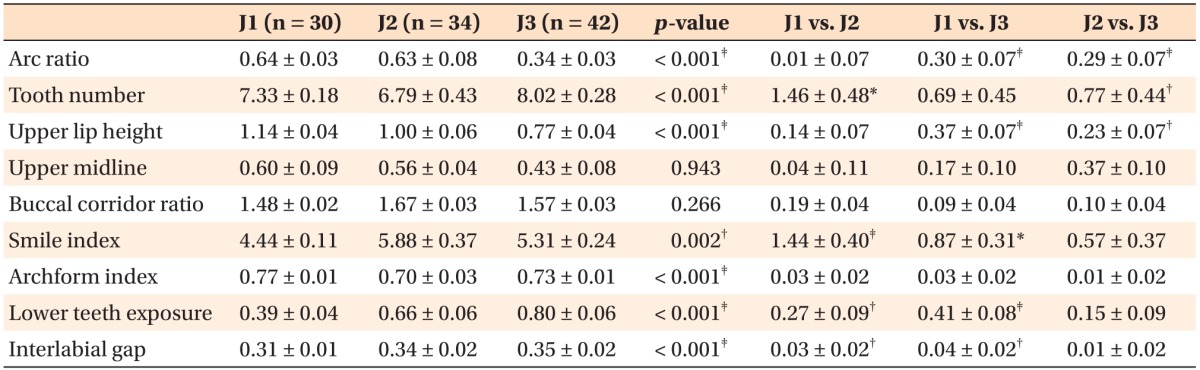
The smile analysis showed that, except for the upper midline and buccal corridor ratio, all of the smile measurements differed significantly among the groups before orthodontic treatment (Table 3). Tooth number, smile index, and lower teeth exposure differed significantly between Groups J1 and J2. Arc ratio, upper lip height, smile index, lower teeth exposure, and interlabial gap differed significantly between Groups J1 and J3. Significant differences were observed in arc ratio, tooth number, and upper lip height between Groups J2 and J3.
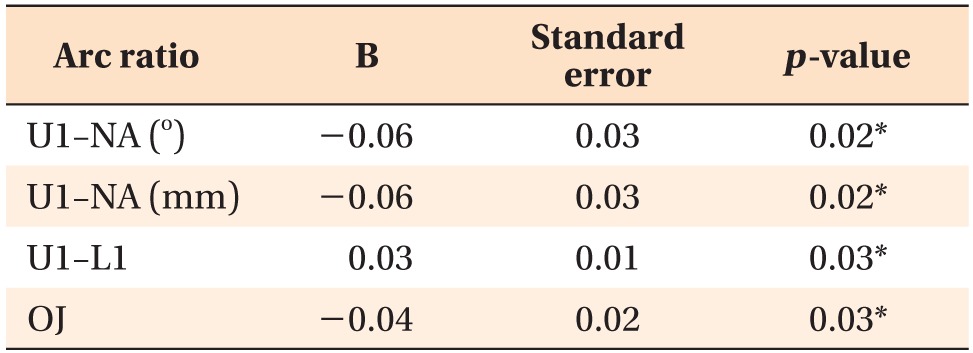
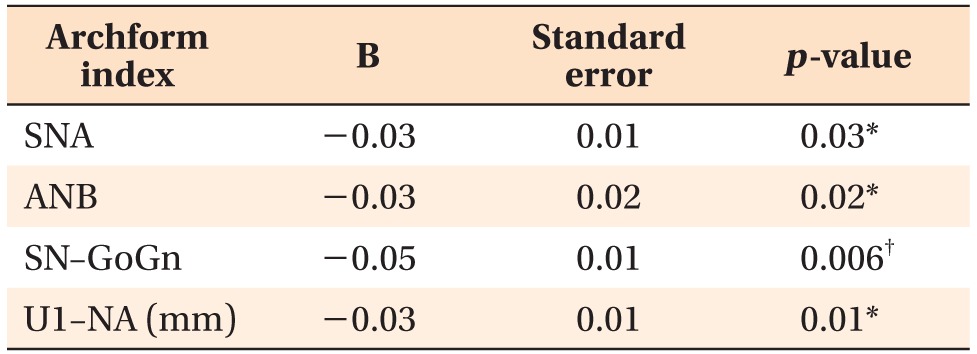
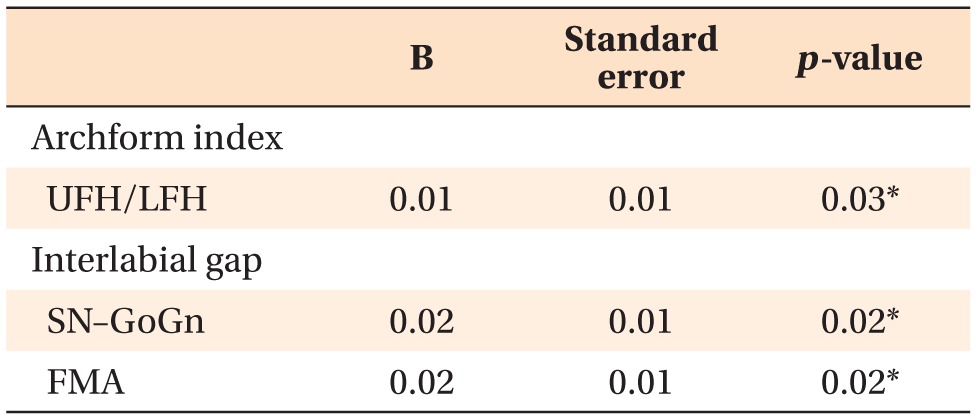
Multiple linear regression analysis for Group J1 revealed that arc ratio was positively correlated with U1-L1 and negatively correlated with U1-NA (°), U1-NA (mm), and OJ (Table 4). In Group J2, arch form index was negatively correlated with SNA, ANB, SN-goniongnathion (GoGn), and U1-NA (mm) (Table 5). In Group J3, arch form index was positively correlated with UFH/LFH, and interlabial gap was positively correlated with SN-GoGn and Frankfort-mandibular plane angle (FMA) (Table 6).
DISCUSSION
In this study, we quantitatively assessed the relationship of smile esthetic variables with various types of anterior OJ malocclusion, and identified the cephalometric factors affecting smile measurements. To the best of our knowledge, this is the first study to assess variations in smile variables by considering the horizontal relationship of dental malocclusion. Although Campbell et al.17 reported that an increased OJ (6–10 mm) influenced the magnitude of smiling, they did not investigate whether variations in OJ affected other smile variables. In literature, the assessment of smile in different types of malocclusions has rarely been reported. Although Yu et al.11 initially classified their study subjects as having Class I, Class II, or Class III malocclusions, the subjects were ultimately pooled together when a subjective attractiveness evaluation was performed. The patients included in the current study were classified into three groups according to OJ. We evaluated the cephalometric and smile measurements separately, and investigated the variations in smile variables between the different types of malocclusion.
Thus far, various investigative methods have been adopted to investigate smile esthetics; they have generally been divided into two types of evaluation. The methodology of smile assessment involving evaluators is called subjective evaluation. Esthetic preferences are typically measured using ordinal and interval scales because they represent a ranked order of assessment from least preferred to most preferred.18 The limitation of subjective evaluation is that the perception of esthetics varies from person to person and is influenced by personal experiences and social environments.14 Many esthetic concepts regarding the face and smile are based on the opinions of authors instead of on reliable scientific methods.19 The other evaluation method, called objective evaluation, involves quantifying smile variables from photographs.57 We used objective evaluation to analyze smile characteristics. The definition of each smile variable was a ratio (a/b%) used to minimize errors and increase reliability. Comparing smiles among different patients or over time in one patient is very useful.20 The gender distribution in each group was not balanced. However, because the gender distribution was not statistically different between the three groups (chi-square = 2.1617, p = 0.3393), we did not include it in further analysis.
The cephalometric analysis (Table 2) revealed that the mandibular position differed significantly between Groups J1, J2, and J3. This finding was consistent with their OJ discrepancy. The cephalometric measurements indicated that the patients in Group J2 had a skeletal Class II relationship and mandibular retrognathism as well as a high mandibular plane angle, and that those in Group J3 had skeletal Class III relationship and mandibular prognathism. The angle and distance of U1-NA and L1-NB indicated that most of the patients in Group J1 had dentoalveolar bimaxillary protrusion malocclusion.
The smile analysis (Table 3) results showed that different types of malocclusion resulted in different types of smiles. Regarding the malocclusion in Group J1, according to multiple linear regression analysis (Table 4), the arc ratio was significantly influenced by four of the cephalometric factors, particularly the angle and distance of the maxillary incisors. Sarver and Ackerman20 had reported that incisor proclination dramatically affects incisor display. Flared maxillary incisors tend to reduce incisor display, while upright maxillary incisors tend to increase it. Lan et al.21 found that the smile arc is flatter at a greater inclination of the maxillary incisor, and narrower at a lower inclination. The quantitative data obtained in our study supported these qualitative descriptions. Because most of the patients in Group J1 had dentoalveolar bimaxillary protrusion, their maxillary incisors were more proclined, and their smile arc was flatter. Therefore, the arc ratio was negatively correlated with the distance and angle of the maxillary incisors and OJ, and positively correlated with the U1-L1 angle.
Regarding the malocclusion in Group J2, according to multiple linear regression analysis (Table 5), the arch form index was significantly influenced by four of the cephalometric factors. A possible explanation is that most of the patients in Group J2 had skeletal Class II relationship and mandibular retrognathism, as well as a high mandibular plane angle. Vertical growth patterns are correlated with the transverse growth of the upper arch in skeletal Class II. When the mandibular plane angle increases, the upper arch form tends to be narrower.22 In addition, Giuntini et al.23 had reported that the upper intermolar width in Class II malocclusion was significantly less than that in Class I malocclusion. The results of our study are consistent with their findings. However, according to the multiple linear regression analysis of Group J3 (Table 6), the interlabial gap was significantly influenced by the mandibular plane angle. Our results revealed that the interlabial gap became wider with an increase in the mandibular plane angle in Group J3.
Although our study is a retrospective study, the inclusion of subjects was randomized in order to decrease the sample bias. However, smile analysis is complex and difficult. Because a smile is not a fixed feature, dynamic alteration may be influenced by several factors. The advantage of using a frontal facial photograph for analysis in this study was that the process was simple and cost-effective, and the number of participants could be easily increased.24 In addition, such photographs are usually available in orthodontic clinical practice. However, it has been reported that evaluation of smile esthetics during facial animation using this method poses a major difficulty in precise capture of repeatable and reliable image at one or multiple time points.25 Another limitation was the difficulty in obtaining a natural smiling photograph. Because the patients did not have a well-aligned occlusion before orthodontic treatment, they might have felt shy in smiling.24 Moreover, several factors may not be easily visible in frontal smile photographs. The problem of an excessive positive or negative OJ is not as apparent in frontal smile photographs as it is in oblique and lateral smile photographs.20 In the future, different views of smile photographs may have to be assessed to ensure a comprehensive smile analysis.
Recently, numerous studies202627 have used dynamic recording of smile by digital videography. It has been noted that standardized digital videography provides the clinician with a wider range of images for selecting the parameters of lip-tooth relationship during facial animation, and that it is possible to select matching images at different time points from these multiple frame galleries to effectively compare the “same” posed social smile. Undeniably, error is associated with selection of the appropriate still frame representing the posed social smile; similarly, a photograph taken of the smile has error associated with it.28 Schabel et al.28 found that there is no clinically significant difference between the images of smiles of subjects captured by clinical photography and the smiles of the same subjects obtained from digital video clips.
We used nine smile variables to investigate the differences between smiles in various types of malocclusion, but these nine variables could not represent all smile characteristics. Although each smile variable was defined as a ratio (a/b%) in order to minimize errors, some factors may not have been accounted for while evaluating these ratios. Our results showed that the horizontal discrepancy of anterior teeth (OJ) may be the major variable influencing the smile pattern in different types of malocclusion. In orthodontic clinical application, establishment of an optimal horizontal anterior teeth relationship is the key to improving the smile characteristics. We speculate that the vertical discrepancy of anterior teeth (OB) may also influence the smile. We plan to investigate this issue in future studies.
This study confirmed that the smile pattern varies between different types of malocclusion, and that the smile is influenced by skeletal pattern and dental projection. Orthodontists must take into account the smile esthetics during diagnosis, treatment planning, and treatment mechanisms before orthodontic treatment. However, analysis of dynamic facial characteristics by using 2-dimensional photographs of patients is difficult.202930 Further research is required to investigate smile features and advance the knowledge in this field.
CONCLUSION
The findings of this study reveal the following:
Most of the smile variables (arc ratio, tooth number, upper lip height, smile index, archform index, lower teeth exposure, interlabial gap) differed significantly among different types of anterior OJ malocclusion.
Some of the smile characteristics were related to the cephalometric measurements in different types of anterior OJ malocclusion.
The smile may be influenced by skeletal pattern and dental procumbency.
The horizontal discrepancy of anterior teeth (OJ) may be the major factor affecting the smile pattern in different types of anterior OJ malocclusion.

 XML Download
XML Download