

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Titanium and its alloys are considered good metallic implant materials because of their high corrosion resistance, excellent biocompatibility with oral tissues, and mechanical strength.1 Titanium implants are widely used for skeletal anchorage in orthodontic treatment because of their many advantages such as flexibility in site placement, low cost, simple implant procedure, and less patient trauma.2
Numerous studies have assessed the risk factors associated with miniscrew failure. One complication is miniscrew fracture during placement or removal, which sometimes makes it difficult to remove the fragment from inside the bone.3 Another complication is periscrew inflammation, which can damage the bone surrounding the neck of the miniscrew.345
Fluoride-containing adhesives, pastes, and oral rinses are commonly used to prevent dental caries and tooth demineralization in orthodontic treatment.67 Clinical evidence indicates that treatment using fluoridecontaining materials is beneficial for managing and preventing white spot lesions during fixed orthodontic treatment.8 However, many reports have suggested that fluoride causes corrosion of titanium implants, and this can lead to implant fracture due to stress corrosion.9101112 A solution containing more than 30 ppm hydrofluoric acid can cause corrosion by destroying the oxidation film of titanium.131415 Therefore, more focus should be placed on dissolved metal ions such as aluminum and vanadium ions that may cause cytotoxic effects, adverse tissue reactions, and stimulate carcinogenic reactions.16171819202122232425 The corrosion of titanium also has a potential effect on general health. Nevertheless, information related to the effects of these oral rinses on the corrosion behavior of titanium alloy miniscrews is lacking. Therefore, a well-controlled study on this issue is necessary.
The purpose of this study was to examine the effects of commercially available fluoride-containing oral rinses on the corrosion behavior of titanium alloys, which are the main components of orthodontic miniscrews. The null hypothesis of this study was that there would be no significant difference in the corrosion behavior of titanium alloys in oral rinses containing different levels of fluoride.
Go to : 
MATERIALS AND METHODS
Materials
Twenty-five commercial titanium alloy (Ti-6Al-4V) circular plates (TC4; Sheng Xinyuan Titanium Industry Co., Ltd., Baoji, China) were examined under each set of test conditions in this study (n = 5 plates for each condition). The alloy specimens (diameter, 15 mm; thickness, 2 mm) were used for electrochemical corrosion tests and determination of surface characteristics. They were polished with #400-, #600-, #800-, #1,200-, and #2,000-grit silicon carbide sandpaper and mirrorpolished using a 1-micron diamond grinding paste. They were then ultrasonically cleaned for 10 minutes in alcohol and 10 minutes in distilled water. Electrochemical tests were performed using a VersaSTAT3 potentiostat (Model 300; AMETEK, Inc., Berwyn, PA, USA), which was coupled with the VersaStudio 2.43.3 software (AMETEK, Inc.) used for electrochemical control and data analyses.
Test solutions
The four commercially available oral rinses (pH, 4.17–6.30; fluoride concentration, 3.92–260 ppm; volume, 400 mL) that were used as the test solutions and saline, which was used as the control solution, are presented in Table 1. All products were subjected to pH measurement and a fluoride ion concentration test. The temperature of the test solutions was maintained at 37℃ ± 0.1℃ during the electrochemical analysis of the titanium alloys.

Open-circuit potential measurements
The counter electrode was graphite and the reference electrode was a potassium chloride (KCl)-saturated silver/silver chloride (Ag/AgCl) electrode. The potential of the reference electrode was denoted by E (Ag/AgCl) = E (saturated hydrogen electrode) + 197 mV. The test samples were connected as the working electrode and immersed for 2 hours in the test solution. Based on the findings of a previous study,26 the 2 hours of immersion used in this study corresponds approximately to the use of an oral rinse for 6 months (i.e., 40 seconds daily), which is similar to the normal orthodontic treatment time with a fixed miniscrew appliance. The exposure area of the working electrode was 0.95 mm2.
Potentiodynamic polarization measurements
After the open-circuit potential (OCP) was monitored for 2 hours, a potentiodynamic polarization measurement was conducted. Because of the low OCP value measured on titanium in the test solutions, the potentiodynamic polarization was initiated at −1.5 V and continued until 0.5 V, at a scan rate of 10 mV/s.27 The potentiodynamic polarization was subsequently subjected to the Tafel tests arranged from an Eocp (OCP/natural electrode potential) of −250 mV to +250 mV to identify the corrosion current density (Icorr), the corrosion potential at Icorr (Ecorr), and the corrosion rate at Icorr (Rcorr).14
Surface analysis
The morphology of the titanium alloy surfaces before (i.e., control) and after the electrochemical measurements were examined under a field-emission scanning electron microscope (FE-SEM) (JSM-7001F; JEOL, Ltd., Tokyo, Japan).
Statistical analysis
After conducting the Shapiro–Wilk normality tests, one-way analysis of variance with the post-hoc Tukey test was used to compare the corrosion resistance of the titanium alloy samples immersed in the fluoride-containing solutions to that of the control alloy samples immersed in saline. All data analyses were conducted using IBM SPSS Statistics ver. 23.0 (IBM Corp., Armonk, NY, USA) at a significance level of 0.05.
Go to :
RESULTS
Open circuit potential measurements
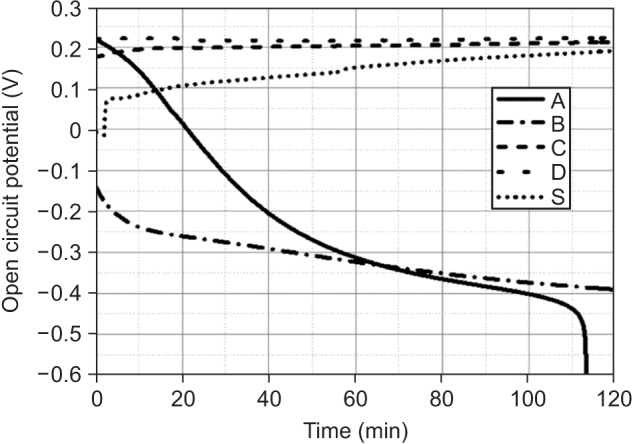
The changes in the OCP versus time in the four oral rinses containing different amounts of fluoride ions and in saline are shown in Figure 1. Under the open-air condition, the OCP values decreased more significantly over time in solutions A and B than in the other solutions. The OCP values on the curve of solution A decreased more rapidly than did those on the curve of solution B. The curves of solutions C and D revealed stable OCP values (to approximately 0. 2 V) in 2 hours. The OCP value of saline increased quickly during the first few minutes, and later gradually increased to nearly 0.2 V in the remaining time.
Potentiodynamic polarization measurements
The potentiodynamic polarization curves recorded for the titanium alloy samples in saline and the four oral rinses containing different fluoride concentrations and different pH values are shown in Figure 2. The graph was drawn with the minimum values in each group.
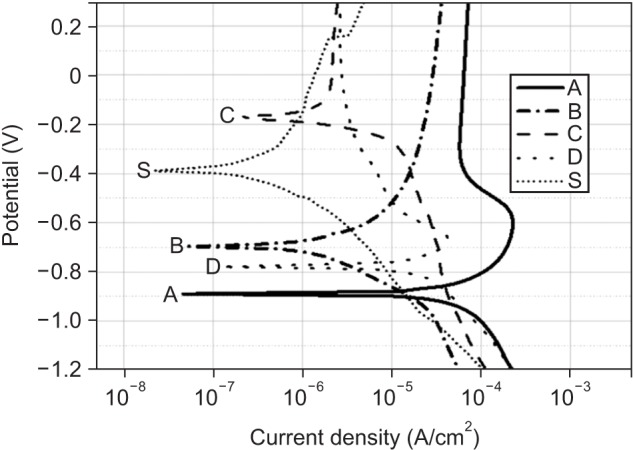
A marked difference was observed in the corrosion potential between the five solutions. The corrosion potential of the solutions in sequence from high to low was as follows: solution C, saline, solution B, solution D, and solution A.
When a stable passive current plateau occurred, the values of current density in solutions A and B were higher than those of solutions C and D. The value of solution A was higher than that of solution B. In addition, the values of current density in solution C, solution D, and saline were similar.
Five samples in each solution were tested. The means and standard deviations of Icorr, Ecorr, and Rcorr are shown in Table 2. Statistically significant differences were observed between the five solutions in Icorr, Ecorr, and Rcorr (p < 0.05).
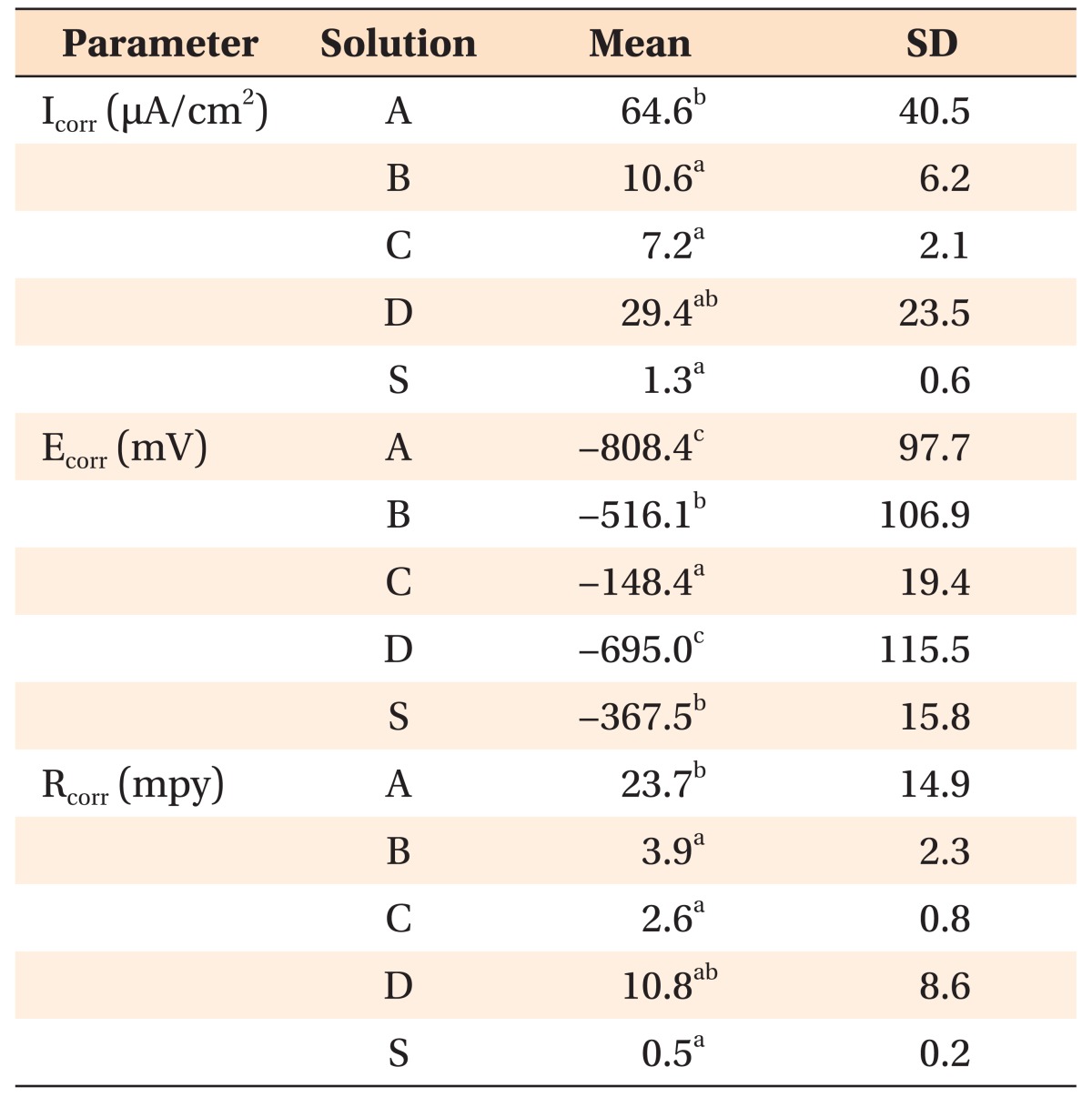
Table 2
Means and standard deviations (SD) of Icorr, Ecorr, and Rcorr in four oral rinses and saline
Icorr, corrosion current density; Ecorr, corrosion potential at Icorr; Rcorr, corrosion rate at Icorr.
The same superscript letters indicate no statistically significant difference between the groups (p > 0.05). Increasing group mean values are expressed in ascending alphabetical order.
Four oral rinses containing (A) 260 ppm fluoride, (B) 178 ppm fluoride, (C) 117 ppm fluoride, (D) 3.92 ppm fluoride, and (S) saline.
![]()
Statistically significant differences were also observed in the Icorr between solutions A and B, solutions A and C, and solution A and saline (p < 0.05). No statistically significant difference was observed in the Ecorr between solutions A and D and between solution B and saline. Moreover, statistically significant differences were observed in the Rcorr between solutions A and B, solutions A and C, and solution A and saline (p < 0.05).
Surface analysis
The surface morphology of the titanium samples assessed using FE-SEM after the electrochemical corrosion tests (i.e., OCP and potentiodynamic polarization) are shown in Figure 3. Sample A primarily had scratches and defects originating from the grinding and polishing operation performed during the pretest. No clear signs of any general or localized corrosion were observed on its surface. However, the samples in the other four oral rinses and in saline had localized corrosion. The sample in solution A had many more defects, crevice corrosion, and pitting than did the other samples. The sample in solution B also had some defects and pitting, but not as much as in solution A. The samples in solutions C and D and in saline had lesser pitting than did the samples in solutions A and B.
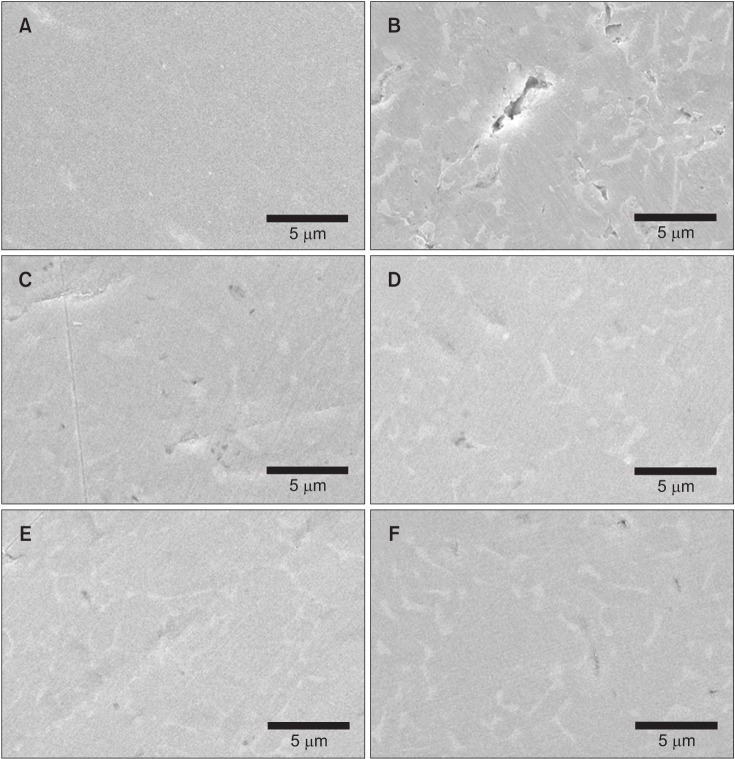 | Figure 3Surface morphology of the titanium samples under a field-emission scanning electron microscope after the electrochemical corrosion tests (magnification, 5,000×). (A) Micrograph of a sample before the electrochemical tests. Micrographs of samples after treatment with (B) solution A (260 ppm fluoride), (C) solution B (178 ppm fluoride), (D) solution C (117 ppm fluoride), (E) solution D (3.92 ppm fluoride), and (F) the saline solution. Scale bars = 5 µm.
|
Go to :
DISCUSSION
To replicate clinical conditions, the present study used some commercially available oral rinses as the experimental solutions and saline as the control solution. A previous study28 showed that pure titanium and titanium alloys may easily corrode in an acidic environment, even at low fluoride concentrations.
According to the findings of the present study, as shown in Figure 1, the OCP values of the titanium alloy decreased in solutions A and B, and especially so in solution A. A previous study29 showed that a decrease in the OCP of a metallic material in a certain environment revealed an increase in its chemical reactivity, and a subsequent predisposition to corrosion. Thus, we can infer that the chemical reactivity of the titanium alloy in solutions A and B increased with a probable change in the properties of the titanium oxide surface film. The alloy samples in solutions C and D revealed a similar and relatively stable chemical reactivity at a noble potential. The corrosion potential gradually increased over time in saline, suggesting that the alloy samples maintained good corrosion resistance.
As shown by the anodic polarization curve, when a stable passive current plateau occurred, the current density values in solutions A, B, and C decreased in sequence with increasing fluoride concentration (Figure 2). The greater the current density, the greater the dissolution of metallic ions. This could indicate that the corrosion resistance of the titanium alloy decreases as the fluoride concentration increases.
The Ecorr values of the potentiodynamic polarization test revealed statistically significant differences between each solution pair, except between solutions A and D and between solution B and saline. In solutions A, B, and C, the mean Ecorr values decreased in sequence with increasing fluoride concentration (Table 2). This result indicated a reduction in the corrosion resistance of the titanium alloy as well as in the stability of its passive film when the fluoride concentration increased.
The mean Rcorr value also increased with increasing fluoride concentration, except in solution D. This finding suggested that the corrosion rates of the titanium alloy in solutions A, B, and C increased with increasing fluoride concentration.
The mean Ecorr was higher in solution C than in saline, even though the mean Icorr and mean Rcorr were much lower in saline than in solution C. An interpretation of this finding is that the actual corrosion rate was higher in solution C than in saline.
The pH values of solutions A and B were similar at approximately 4.4 (Table 1). The comparison of solutions A and B showed that the corrosion resistance of the titanium alloy decreased with increasing fluoride concentration. Previous studies152730 have shown that the decrease in the corrosion resistance of titanium or titanium alloys was more significant in a solution containing a greater concentration of fluoride at the same pH, and that a solution containing a higher concentration of fluoride could dissolve more metal ions.
As for solution D (which has no fluoride, according to the manufacturer), there may be several reasons why it reduced the corrosion resistance of the titanium alloy. There may have been a little fluoride in solution D, even though it was not listed by the manufacturer. The pH value in solution D was the lowest among the four oral rinses. Moreover, although no statistically significant difference was observed between solutions A and D, a comparison of the mean Ecorr showed that the sample in solution D had a higher value than did the sample in solution A. A previous study28 showed that a solution with a lower pH value induced a lower corrosion resistance in the titanium alloy at the same fluoride concentration. Solution D had a lower pH value than did solution A; despite this, the corrosion resistance of the alloy sample was higher in solution D than in solution A, which contained more fluoride. This result may be related to the concentration of fluoride in the oral rinses. Previous studies2731 have also demonstrated that a solution with a low pH value and a lower fluoride concentration could have induced a better corrosion resistance in the titanium alloy than did a solution with a higher fluoride concentration and a higher pH value. The fluoride content itself may be crucial for corrosion. Another possibility is that some other components in the rinses could have reduced the corrosion resistance.
According to the surface morphology of titanium samples observed under FE-SEM after electrochemical corrosion tests (Figure 3), the samples in solution A showed many more defects, crevice corrosion, and pitting corrosion than did the other samples. The greater the extent of pitting corrosion and crevice corrosion present on the surface of the samples, the more the corrosion. The surface of the alloy in saline also seemingly had some slight crevice corrosion and pitting corrosion, but this may have been caused by the autocatalytic reaction of chloride ions. When a metal surface has a pit or crevice, the quantity of metal cations increases inside the defect than in the other parts of the metal because of the lack of oxygen. To maintain a charge balance, more chloride ions move to the pit or crevice and cause an autocatalytic reaction. This process can cause metal corrosion. The results in Figure 3 could consequently indicate that the greater concentration of fluoride caused greater corrosion in the samples.
The results of the study partially rejected the null hypothesis. Among the tested oral rinses, except solution D, the more the fluoride content was, the lower was the corrosion resistance of the titanium alloy sample. Therefore, the long-term use of oral rinses with a high fluoride concentration is likely to influence the properties of titanium orthodontic appliances such as titanium-molybdenum alloy wires, miniscrews, and brackets.
Previous studies2731 have shown that a solution with a low pH value and no fluoride could induce a better corrosion resistance in the titanium alloy than does a solution that has a low fluoride concentration and a high pH value. If there had been another control group with a fluoride-free acidic solution in this study, it may have clarified the crucial impact of fluoride content on corrosion resistance. In addition, the evaluation method and small sample size may have limited the applicability of the results of this study. Future studies should aim to have larger sample sizes and use more clinically relevant methods to verify the current findings.
Go to :
CONCLUSION
Fluoride has been used for preventing caries during orthodontic treatment. However, commercially available oral rinses that have a high concentration of fluoride and a low pH value may reduce the corrosion resistance of titanium alloys used in dental appliances such as orthodontic titanium miniscrews and brackets.
Go to :
 XML Download
XML Download