

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Previous studies have reported that all healthy people exhibit some degree of facial asymmetry, including individuals whose faces are perceived as normal.12 Subtle facial asymmetry is not noticed by the individual or by those who frequently see him or her because facial asymmetry is often present in the normal craniofacial complex.34 However, patients with facial asymmetry requiring orthodontic treatment and/or orthognathic surgery are more focused on their appearance and may be more concerned about facial asymmetry. Treatment can also affect asymmetry, as some patients believe that asymmetry develops or progresses during or after treatment because they were not aware of it before treatment.5
Lip-line cant is one of the most noticeable features in patients with facial asymmetry and is usually associated with hard- and soft-tissue asymmetry.6 Hard-tissue asymmetry results in maxillary occlusal plane cant and is defined as an inconsistency between the amounts of dentition and gingival exposure. Soft-tissue asymmetry is determined by the difference in commissure height bilaterally.7 Padwa et al.8 reported that when the frontal occlusal plane cant exceeds 4° on posteroanterior cephalograms, 90% of the general population notices the cant. Moreover, Hwang et al.9 reported that preoperative lip-line cant was significantly correlated with menton deviation in one-jaw orthognathic patients.
Many previous studies reported associations among labial morphology or lip aesthetics, sex, and aging.1011121314 However, to our knowledge, few studies have investigated the correlations between lip-line cant, sex, and age in Asian adults who vary widely in age. Such metrical differences between sex and age have practical importance in several areas associated with facial aesthetics, particularly in situations where the main task consists of adequately reproducing the anatomical structures according to a specific biological profile.10
Therefore, the aims of this study were to assess the direction and degree of lip-line cant in Korean adult orthodontic patients and to identify the effects of sex and age on changes in cant severity. Our null hypothesis was that no significant correlations exist between the age and sex of patients and the direction and degree of lip-line cant.
MATERIALS AND METHODS
Samples
The present study was a cross-sectional retrospective evaluation of 585 adults (> 18 years of age) who visited a private clinic between January 2010 and May 2013. The inclusion criteria were as follows: age > 18 years; complaints of chin deviation; no congenital malformations such as cleft lip and/or palate, or any disease that might affect craniofacial asymmetry; and standardized frontal photographs acquired before treatment that were of sufficient quality for evaluation. Patients with a history of orthognathic or cosmetic surgery in the facial region were excluded. Written informed consent was obtained from each participant.
Methods
A frontal photograph and a posteroanterior cephalo gram were obtained for diagnosing the facial asymmetry of each subject. To acquire the images, the subject was seated in an upright position with the Frankfort horizontal plane parallel to the floor, as determined by using the vertical line of Gonzalez-Ulloa (a vertical line dropped from the nasion perpendicular to the Frankfort horizontal plane) or a line drawn from the lower lip with the head in the Frankfort plane. All facial photographs were taken in the same room with the same camera (G12; Canon, Tokyo, Japan).
The collected data were delivered to a professional programmer, who designed custom software in Python 2.7.3 (Python Software Foundation, Beaverton, OR, USA). Using this software, the degree of lip-line cant was evaluated by measuring the angles between the interpupillary line and the intercommissure line. The degree of lip-line cant was recorded as an absolute value plus the direction of the deviation (the right commissure was higher than the left commissure or vice versa) (Figure 1).
To investigate the relationship between the menton deviation angle and lip-line cant, posteroanterior cephalograms were taken with a metal ball attached to each ear rod in the head holder as the reference to ensure the Frankfort horizontal plane was parallel to the floor. Images were obtained with a Pax-Uni3D digital X-ray system (Vatech, Hwaseong, Korea) and digitized with VCeph 7.0 (Osstem, Seoul, Korea). The menton deviation angle was measured as the angle formed by the anterior nasal spine-to-menton line and the midsagittal line (crista galli to anterior nasal spine). The absolute value was used for statistics irrespective of the direction of deviation (Figure 2).
Each patient's lateral cephalometric skeletal relationship was classified into sagittal classes (I, II, or III) according to the ANB, A point-Nasion-B point angle: Class I, 0°-4°; Class II, > 4°; Class III, < 0°.15 The reproducibility of all measurements was evaluated with duplicate measures of a subset of randomly collected photometric and cephalometric data from the films of 100 patients that were taken two weeks apart. To calculate the reproducibility between the two readings, Dahlberg's formula was used. The error ranged from 0.1° to 0.2° for both the lip-line cant and menton deviation angle, which were not statistically significant.
Statistical analysis
The Kolmogorov-Smirnov test revealed that the data were not normally distributed; thus, non-parametric tests were used in the subsequent analyses. Descriptive statistics such as the mean and standard deviation (SD) were used to verify the general characteristics of the subjects. Differences in the direction of lip-line cant were analyzed with χ2 tests. The Mann-Whitney U test and the Kruskal-Wallis test were implemented to assess mean differences in the degree of lip-line cant and menton deviation angle according to sex, age, and skeletal classification. Correlations between lipline cant and sociodemographic factors and craniofacial measurements were assessed with the Spearman rank correlation. To evaluate the strength of the correlation, r > 0.40 was considered to indicate a moderate to strong correlation, while r < 0.40 was considered to indicate a weak correlation. In the multiple linear regression analysis, we conceptualized lip-line cant as dependent variables. A forward selection process with entry into the model depending on the significance of the F value was performed. If necessary, we dummy-coded the categorical variables for the regression analysis. All statistical analyses were performed with IBM SPSS for Windows version 21.0 (IBM Korea Inc., Seoul, Korea).
RESULTS
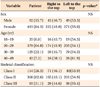
Complete data were obtained for 585 adults (92 men and 493 women) with a mean age of 27.0 years (range, 18-48 years); 84.3% of participants were women. Regarding the patients' skeletal classifications, 154 patients (26.3%) were Class I, 366 patients (62.6%) were Class II, and 65 patients (11.1%) were Class III. The direction of lip-line cant did not differ according to sex, age, or skeletal classification (Table 1).
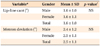
Our patients had an average of 1.6° of lip-line cant (SD, 1.0°) before orthodontic treatment. The average menton deviation angle was 2.5° (SD, 1.1°). Neither lip-line cant nor menton deviation significantly differed between the sexes (Table 2).
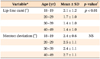
The mean degree of lip-line cant in patients aged 18-19 years was 2.1° (SD, 1.2°); this value was 1.4° (SD, 1.0°) in patients aged 40-49 years. Middle-aged adults displayed a significant trend toward lower degrees of lip-line cant compared to younger adults (p < 0.01) (Table 3). However, the menton deviation angle was not significantly different between the age groups.
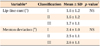
Neither the degree of lip-line cant nor the menton deviation angle differed between the skeletal classification groups (Table 4). However, as shown in Table 5, the degree of lip-line cant showed a weak positive correlation with the menton deviation angle (p < 0.001), as well as a weak negative correlation with age (p < 0.01; correlation coefficients, -0.142 to 0.195).
The multiple linear regression analysis showed that two key factors were significantly associated with lip-line cant after adjusting for sex, age, and other variables. R2 = 0.057 showed weak linear relations and predictability between lip-line cant and age (B, -0.023; standard error [SE], 0.006; p < 0.001) and between lip-line cant and menton deviation (B, 0.193; SE, 0.039; p < 0.001).
DISCUSSION
In the current study, the lip-line cant direction did not differ according to sex, age, or skeletal classification (Table 1). Similarly, Ferrario et al.16 did not show any sex- or age-related differences in either the absolute or percent indices of individual asymmetry. Previous studies indicate that no consensus exists regarding the importance of the side of the facial asymmetry because factors such as sex, age, and race of the investigated subjects differed between investigations and could partly underlie the contrasting findings.1718 However, in the present study, age was weakly, but significantly, associated with the degree of lip-line cant. Specifically, we found that middle-aged adults tended to display significantly lower degrees of lip-line cant compared to younger adults (p < 0.05), but menton deviation was not significantly different between the age groups (Table 3).
Previous studies revealed that skeletal deformities can be hidden by soft tissues such as muscles and skin, which may partly mask underlying imbalances.1920 Lip-line cant is defined as the difference in the vertical heights of both commissures, which are associated with the actions of three muscles: the upward pull from the zygomaticus major and levator anguli oris muscles and the downward pull from the depressor anguli oris muscle.2122 The buccinator muscles also pull the labial commissure and comprise the deep layer of the orbicularis oris muscle.7
Changes in the degree of lip-line cant over time result from decreases in the elasticity of the facial muscles and the loss of facial volume, including bone, muscle, fat, and skin tissue.23 Asian facial skin is usually thicker than that of Westerners; thus, the skin of the midface sags rather than wrinkles due to aging.24 In the face, volume loss due to decreases in the amount of fat tissue is a prominent phenomenon.25 Due to aging, the lateral portions of the lips recede and the distance between the columella and the vermilion border of the upper lip increases, yielding changes in the lip line and lip volume that are characteristic of old age.1326 Older subjects who have sustained photodamage or who smile excessively can develop permanent, deep nasolabial folds that extend from the lateral nasal ala to the commissures of the mouth bilaterally.26 These changes in the muscles, skin, and fat around the mouth appear to play a role in reducing the degree of lip-line cant with aging.
Here, the menton deviation angle was also associated with the degree of lip-line cant (Table 5). Many previous studies have similarly reported that the menton deviation angle and mandibular gonial angle significantly affected lip-line cant.927 Increases in the menton deviation angle under the influence of the depressor anguli oris muscle, which attaches in the mandible, can increase the degree of lip-line cant. For example, to relocate the position of the lip commissure superiorly, the surgeon must manipulate the depressor anguli muscle's attachment point on the mandible via orthognathic surgery.7 However, controlling the amount and direction of muscle change is difficult because the attachment point, thickness, and length of the muscle can be altered by horizontal, sagittal, and vertical movement of the mandible via orthognathic surgery.7
Based on these results, flattening of the lip line may require a minimally invasive surgical operation, usually performed in middle-aged adults, to modify the perioral soft tissues and enhance the labial volume using dermal fillers.1028 Additionally, lip-line cant is more distinct in early adulthood than it is in mid-adulthood, therefore, such lip asymmetry should be noted during treatment planning in young patients with menton deviation. Documenting any existing asymmetry prior to treatment is particularly important since some patients may believe that lip asymmetry developed or progressed during or after treatment if they were not aware of it or were not notified of it by a doctor before treatment. A considerable proportion of lawsuits result from a lack of understanding between doctors and patients rather than from errors in treatment.29 Thus, open communication between doctors and patients regarding asymmetry and the recommended treatment plan is essential.
Some limitations of the current investigation should be considered when interpreting the data. First, the present study was a retrospective and cross-sectional study without sample purity. Evidence regarding the negative correlation between aging and the severity of lip-line cant was lacking due to the cross-sectional design of this study, which may limit our ability to extrapolate these findings to the general population. In the future, investigating longitudinal data from a homogenous sample such as female patients with severe menton deviation (more than 5 mm) and lip-line cant (more than 4°) might be better for assessing causation. Second, the sex ratio was skewed in this study (84.3% female, 15.7% male). Sex may influence the factors analyzed here, as middle-aged women can be affected by asymmetric facial skin viscoelasticity after menopause due to hormonal changes.30 Additional prospective studies are needed to further evaluate the relationships among lip-line cant, aging, and the craniofacial complex using a homogenous sample.
CONCLUSION
Sex, age, and skeletal classification were not associated with differences in the direction of lip-line cant in our study on Korean adult orthodontic patients. However, the degree of lip-line cant showed a weak positive correlation with the menton deviation angle, as well as a weak negative correlation with age that was independent of menton deviation. Specifically, we found that middle-aged adults tended to display significantly lower degrees of lip-line cant than did younger adults.



 XML Download
XML Download