

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Oral health affects people physically, as it is closely related to appearance, enjoyment, eating, speech, taste, and growth.1 In addition, it exerts a strong influence on socialization and social well-being; therefore, the psychological effects of oral health should be evaluated. Disruption to psychological and social functioning, in addition to physical functioning, is important in assessing oral health. In other words, oral health should be defined according to psychological and social well-being as well as physical factors. Traditional measures should be supported using measures of oral health-related quality of life in sociodental approaches to assessing treatment need.2
Increasing demand for orthodontic treatment could be attributed to dental aesthetics and its psychological effects.34 Generally, patient expectations of orthodontic treatment include improvements in appearance, self-image, and social functioning.56 From an orthodontic perspective, malocclusion affects oral function and appearance and exerts a crucial social and psychological impact.37 However, professionals generally evaluate orthodontic treatment need using tools such as normal occlusion and cephalometric measurements, disregarding the impact of malocclusion on patients' oral health-related quality of life (OHRQOL).8
In the last decade, patients' perceptions of aesthetics during orthodontic treatment planning has become an interesting topic from a psychological perspective.79 In addition, the use of OHRQOL measurement tools and occlusal indices has been reported to be effective in predicting orthodontic concerns.10 Questionnaires are frequently used in the assessment of OHRQOL and offer information concerning patients' perceptions of their welfare in relation to particular oral conditions.11 Klages et al.5 developed the Psychosocial Impact of Dental Aesthetics Questionnaire (PIDAQ) to measure orthodontics-related OHRQOL. This self-rating instrument could be also used to assess orthodontic treatment need and evaluate changes in OHRQOL subsequent to orthodontic treatment.45
Prior to using questionnaires in different cultures, the implementation of a translation and validation process that takes the cultural and social aspects of the new region into consideration is essential to measure the same constructs with the same accuracy.7 The PIDAQ has been used widely and translated into several languages, and it has demonstrated good validity and reliability; however, it has not been translation into Turkish.4671213
To our knowledge, there are no psychological scales to assess orthodontics-related OHRQOL published in Turkish. Therefore, a Turkish version of PIDAQ could be the first such scale in this field of research. The aim of this study was to translate the PIDAQ into Turkish, validate the questionnaire, and provide a cross-cultural adaptation.
MATERIALS AND METHODS
Ethical approval was obtained prior to initiation of the study from Ethical Committee of Sifa University (ref.: 251–68). All participants were volunteers and provided written informed consent. Participants were undergraduate students from the Faculty of Medicine of Sifa University (Izmir, Turkey). Despite the convenience in sampling, our sample represented different parts of the country, as the institute is in the third-largest city in Turkey. Dentistry faculty students and foreign citizens were excluded from the study. The exclusion criteria were as follows; 1) previous orthodontic treatment, 2) missing or fractured teeth in the anterior region, 3) discoloration in the anterior region, and 4) craniofacial anomaly. In total, the study included 284 individuals, of whom 24 were excluded because of missing data or the provision of more than one answer per questionnaire item. Therefore, the analysis included data from 260 students. The scales were administered in random order, but the informed consent form always appeared first.
Description of the Turkish version of PIDAQ
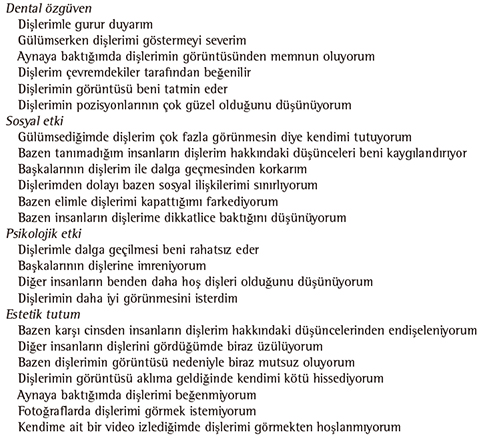
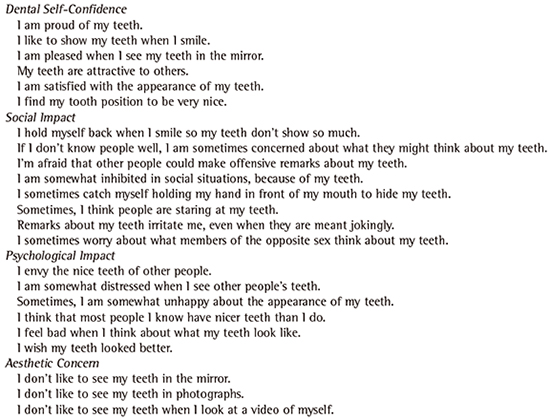
The PIDAQ is a 23-item psychometric scale composed of four subscales divided according to one positive and three negative domains: aesthetic concern (3 items), psychological impact (6 items), social impact (8 items), and dental self-confidence (6 items). Responses are provided using a five-point Likert scale ranging from 0 (not at all) to 4 (very strongly), which represents the extent of the impact of dental aesthetics on quality of life.5
Translation
The permission required to translate the PIDAQ into Turkish was received from one of the developers of the scale (Dr. Andrej Zentner) via e-mail. The scale was translated to Turkish by an orthodontist and a linguist. Another orthodontist and a psychiatrist, who were fluent in English and Turkish, produced and evaluated the first Turkish translation (Turkish Translation I).
Back translation
Assessment of the versions was performed using a double-blind process involving the translator and back translator. A linguist, who was a postgraduate student with no knowledge of the original English questionnaire and familiar with quality-of-life terminology, back translated the Turkish version of the PIDAQ into English. A committee composed of a native English speaker, who was fluent in Turkish, and two linguists compared the original and back-translated versions. Turkish Translation II was developed based on the committee's suggestions and proposals (Appendix 1 and 2).
Cross-cultural adaptation
A committee consisting of two orthodontists, two postgraduate students, a dentist, and a psychiatrist, all of whom were fluent in English and familiar with quality-of-life terminology, were asked to evaluate the scale with respect to cultural relevance, purpose, and clarity. Semantic and conceptual equivalence were assessed once the final revision and Turkish Translation III were developed.
Pilot study
The final version of the translation was pretested by 30 young adults (14 women and 16 men) aged 18–30 years, from the Sifa University Faculty of Medicine. Interviews were conducted by one investigator (FD), to prevent possible differences in explanations concerning the questionnaire. In congruence with the questionnaires, Turkish Translation III, the final Turkish version of the PIDAQ, did not undergo modification.
Measurements used to assess the validity and reliability of the PIDAQ
All participants were asked to indicate their need for orthodontic treatment.
Aesthetic component of the Index of Orthodontic Treatment Need
The aesthetic component of the Index of Orthodontic Treatment Need (IOTN-AC) was used to determine individuals' self-perception concerning their dental aesthetics. Participants were asked to rate the extent to which 10 black and white photographs of anterior teeth demonstrating varying amount of malocclusion resembled their dentition.14
Perception of Occlusal Scale
The Perception of Occlusal Scale (POS) contains six items that indicate the occlusal traits of the anterior region, with responses recorded using a five-point Likert scale in a similar manner to that of the PIDAQ.7
Retest
Thirty students, who were randomly selected (with the help of nicknames), completed the questionnaires in a test-retest assessment performed three weeks subsequent to pretesting, to determine reliability.
Statistical analysis
The Statistical Package for Social Sciences (SPSS Inc., 17.0, Chicago, IL, USA) was used to analyze all data. A factor analysis of the scale was performed using principal components analysis and varimax rotation with Kaiser normalization, to determine structural validity. The internal consistency of the Turkish version of the PIDAQ was assessed by calculating Cronbach's alpha coefficients for the subscales. Distribution of the variables was assessed via the Kolmogorov-Smirnov method. PIDAQ subscale and total scores were compared with self-reported of the IOTN-AC and POS via an ANOVA and the Kruskal-Wallis test. Test-retest reliability was assessed via Spearman's correlation coefficients using correlations between PIDAQ subscale and total scores for determined using correlations between awareness, and satisfaction. An independent samples t-test was performed to compare PIDAQ scores and self-evaluation of orthodontic treatment need.
To facilitate the interpretation of the results, the scores for items concerning dental self-confidence (items 1–6) were reversed. The level of significance was set at p < 0.05.
RESULTS
The study included 284 individuals, of whom 260 returned questionnaires with no missing data, which were included in the analysis (age range, 18–30 years; mean age, 20.50 ± 1.9 years). Sex distribution was almost equal: the proportions of men and women were 47.3% (n = 123) and 52.7% (137), respectively. A need for orthodontic treatment was reported by 96 individuals (36.9%).
Cross-cultural adaptation
Subsequent to the implementation of two changes via the translation process, the translation committee considered the Turkish translation of the PIDAQ semantically and conceptually equivalent to the original. Therefore, cross-cultural adaptation resulted in a tool that was ready for use.
Construct validity
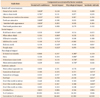
The Kaiser-Meyer-Olkin measure of sampling adequacy was 0.901, and the Bartlett's test of sphericity was significant (2,740.1; p < 0.001). These results showed that the variables were within the normal range and appropriate for inclusion in factor analysis. Four factor structures were extracted in an explanatory factor analysis, with the item factor loadings ranging from 0.380 to 0.868. Sixty-two percent of the four subscale variance reproducing the original PIDAQ. Few questions were shuffled among domains various factor loadings with components are shown in Table 1.
Reliability
Cronbach's alpha internal consistency coefficients for the subscales ranged from 0.534 to 0.904. Cumulative variance for the entire scale was 62.94% (Table 1).
Reproducibility
In the test-retest reliability analysis, Spearman's correlation was used to analyze data from 30 individuals, which were compared with data obtained three weeks later. The test-retest reliability coefficient for the scale was high (r = 0.863, p < 0.001). PIDAQ scores did not differ significantly between the first and second tests.
Discriminant validity
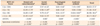
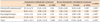
PIDAQ subscale and total scores differed significantly according to IOTN-AC and POS scores (Tables 2 and 3) and self-reported orthodontic treatment need (p ≤ 0.001; Table 4). Men exhibited significantly higher scores relative to those of women, who did not express a need for orthodontic treatment via the dental self-consciousness subscale (p < 0.001; Table 4).
DISCUSSION
Quality of life is commonly assessed via questionnaires, which should be verified for cross-cultural adaptation when the original and translated versions are comparable.15 Questionnaires are suitable for use in different cultural contexts only when they demonstrate good psychometric properties. The cultural adaptation approach used in the translation and validation was proposed by the International Quality of Life Assessment Project,16 to establish the Turkish version of the PIDAQ. According to the results of this study, the PIDAQ's internal consistency, factor structure, and correlations with other scales indicated that the scale is a valid and reliable assessment tool for use in the Turkish culture.
The study sample was homogenous with respect to sex and age. All participants were Faculty of Medicine students; therefore, the sample constituted a well-educated group. Dentistry students and individuals with experience of undergoing orthodontic treatment were excluded from the study, to prevent the inclusion of individuals with knowledge concerning orthodontics and ideal facial aesthetic norms.
To evaluate the equivalence of different language versions of a questionnaire, conceptual, semantic, technical, and psychometric issues require consideration.7 This meticulous process includes the following steps: translation, back translation, cultural adaptation, and pretesting. In this study, a translation committee composed of orthodontists, a psychiatrist, linguists, and a native English speaker performed translation and back translation, to ensure excellent translation and improved understanding and detect potential problems. Back translation showed that the translated version of the PIDAQ was very similar to the original. Similar processes were used in previous studies involving the translation and validation of the PIDAQ in different languages.6713 Similarly, the pilot study showed good results and indicated that the quality of the translation was satisfactory.
Factor analysis is used to evaluate construct validity.7 Five components were extracted in principal component factor analysis with orthogonal rotation. Two components included only two items. One of the Cronbach's alpha values for the components was somewhat low (0.391), and some items did not demonstrate sufficient factor loading in the analysis. Factor analysis then tried fixing the number of components to four as in the original version, this form gave good item factor loading. The results indicated that the validity and reliability of the Turkish version of the PIDAQ in young adults was structured on four components, as in the original, Spanish, Brazilian, and Italian versions.451213
The first component, dental self-confidence, was reported to have a significant impact on individuals' emotional states and has been found to represent subjective perception of well-being.17 This component demonstrated the highest explained variance of all components and was structured with the same items as those of the original version.5
The second component, social impact, included six items, while the original PIDAQ includes eight items. This component represents potential problems arising in social situations, because one perceives one's own dental appearance as unfavorable. The psychological impact factor loading for "Remarks about my teeth irritate me even when they are meant jokingly" was higher relative to that for social impact. In addition, the aesthetic concern factor loading for "I sometimes worry about what members of the opposite sex think about my teeth" was higher relative to that for psychological impact. This result could demonstrate the importance of the opinions of members of the opposite sex with respect to aesthetic concerns.
In the Turkish version of the PIDAQ, aesthetic concern factor loadings for three items, "somewhat distressed," "somewhat unhappy," and "feel bad," were high. In the original version, these items were included under psychological impact. Therefore, the fourth component included psychological impact and aesthetic concern items. This result is quite similar to that for the Chinese version of the PIDAQ, in which it was known as "aesthetics attitude," defined as a state of mind or a feeling concerning aesthetics. Attitudes toward dental aesthetics could also reflect the need for orthodontic treatment.7 For this reason, the fourth factor was entitled "aesthetics attitude," as in the Chinese version.
Together, the four components accounted for 62.93% of the total variance, which is above the minimum recommended threshold for a stable factor solution.18 Furthermore, the original PIDAQ components exhibited a total variance of 63.28%, which is similar to the findings of a study conducted by Klages et al.5
Cronbach's alpha coefficient should be at least 0.70 for questionnaire reliability.19 Cronbach's alpha coefficients were rather high in Nepalese (0.965–0.988) and Chinese (0.905–0.917) populations, whereas considerably lower values were reported for Spanish (0.768–0.862) and Brazilian (0.75–0.91) populations. Cronbach's alpha coefficient for the Turkish version of the PIDAQ was similar to that for the original.5 Moreover, the internal consistency of three of four subscales in this study were strongly related (0.904–0.806), while the internal consistency for the psychological impact subscale was fair (0.534). Three items were moved from "Social impact" subscale to "Psychological impact" subscale and one item was removed from "Psychological impact" subscale to "Social impact" subscale. Lower internal consistency, relative to that of the original version, could be explained by the disarrangement of items in the psychological impact subscale.
In addition, "Remarks about my teeth irritate me even when they are meant jokingly" in the social impact subscale demonstrated the lowest factor loading of all items (0.380; Table 1), and this decreased the psychological impact subscale's Cronbach's alpha coefficient. This factor has quite similar factor load in social impact (0.317; Table 1) as it is under social impact subscale in the original version. In authors' opinion this item might evaluate in social impact subscale. However, as the psychological impact factor loading was a little higher for this item, it was excluded from the social impact subscale.
The test-retest correlation coefficient for the PIDAQ was high (r = 0.863) and could be considered excellent. Discriminant validity has been assessed using the POS and IOTN-AC in previous studies involving the translation and validation of the PIDAQ.4567 In this study, these scales were used to verify the Turkish Version of the PIDAQ. Significant results indicated that higher PIDAQ values were correlated with higher POS and IOTN-AC values (Tables 2 and 3). Similar results were observed in studies using the same protocol for discriminant validity.456
While the IOTN-AC has been used widely, it does not contain items pertaining to Class III malocclusion. However, Sayin and Türkkahraman20 reported that approximately 11.5% of a Turkish population showed Class III malocclusion. The IOTN-AC has been used to rate deviation from malocclusion in the Turkish population.21 Despite this, failure to examine Class III malocclusion could be a limitation of this study. However, as mentioned above, the IOTN-AC is a widely used international scale. This should be considered when interpreting the results of the current study.
All participants indicated their treatment need and were assigned to one of two groups according to their self-perception of treatment need. PIDAQ subscale and total scores differed significantly between groups, suggesting that the scales differentiated between the two groups with respect to OHRQOL (Table 4). The results showed that men and women differed significantly only in the "no treatment need group," in which men exhibited significantly higher scores for the dental self-consciousness subscale relative to those of women. This result could indicate that although men's levels of dental self-consciousness were higher, their self-perception of orthodontic treatment need was low relative to that reported by women. This outcome is consistent with findings indicating that women show greater dissatisfaction and concern regarding their dental appearance relative to that of men.22 Contrary to the results of this study, men and women did not differ significantly in a study examining the Nepalese version of the PIDAQ.6 This difference could be attributed to cultural and ethnic differences between the two populations.
The PIDAQ was strongly correlated with satisfaction with personal dental appearance and weakly correlated with awareness of malocclusion (Table 4). This result indicated that the study population was particularly concerned with appearance and aesthetics, and the PIDAQ reflected this. This could have explained why awareness of malocclusion is poor in the Turkish population and affected by cultural differences and dental awareness.23
Satisfaction with physical appearance is personal and could depend on patients' psychological circumstances. Occasionally, objective and subjective evaluations of orthodontic treatment need differ. Therefore, one of the limitations of this study was the lack of professional evaluation of orthodontic treatment need using specially developed indices.
This study included university students from one of the largest cities in Turkey (Izmir), and the sample could be considered to involve adequate geographic, cultural, and ethnic diversity, because it included students from different regions of the country; it could therefore be regarded as representative of the general population.
CONCLUSION
The present study was important, as it was the first to examine the validity and reliability of the PIDAQ in a Turkish sample. The study provided a Turkish version of the PIDAQ, which could be a useful tool in the evaluation of the psychosocial impact of malocclusion in young Turkish adults.

 XML Download
XML Download