

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
There is a societal trend towards increased awareness and emphasis on beauty and facial aesthetics. Accordingly, the facial profile is one of the most important factors to consider in orthodontic or orthognathic surgical patients.1 Many studies have assessed anterior-posterior relationships of the maxilla and mandible, because these are critical to determining a patient's profile.2
Steiner3 pioneered the use of angles between A-point and B-point and the sella-nasion (SN) line to evaluate the sagittal relationships of the skeleton. Even today, these measures are the most widely used in the world. McNamara4 implemented the McNamara line, which is a line perpendicular to the Frankfort horizontal (FH) plane passing through nasion. He measured the distances from A-point and Pog to the McNamara line. The McNamara line is meaningful for validation of the anterior-posterior assessment of the maxilla and mandible in mm units. Linear measurements can yield more useful sagittal relationships of the skeleton than angular measurements. Specifically, linear measurements in orthognathic surgery are essential for planning and performing and evaluating skeletal movements. However, there are many clinical situations that do not conform to clinical profiles that are amenable to the use of the FH plane and the McNamara line for orthognathic surgical planning because the FH plane has large inter-individual variability relative to the true horizontal line (THL).56
Consequently, the natural head position (NHP) was introduced as an alternative in the late 1950s, to overcome intracranial references such as the FH plane.7 The NHP has been shown to be highly reproducible and reliable as a craniofacial reference system.89 Other advantages of the NHP are its reflection of the true life appearance, and ease of registration. The nasion true vertical line (NTVL) was reported in 1990, and incorporated the concept of the NHP as a reference line from which to measure the linear distances to A-point, B-point, and Pog.10 Normative linear measurements from A-point, B-point, and Pog to the NTVL in Caucasians have been reported.1011
Recent advances in imaging technology have introduced cone-beam computed tomography (CBCT), a technology that provides multi-dimensional images including those that allow for cephalometric analysis.12 There are many reasons to utilize three-dimensional (3D) CBCT images in dentistry.13141516 1) Measurements are real sizes, without the magnifications or distortions associated with conventional two-dimensional (2D) imaging. 2) Spatial relationships between the craniofacial structures are shown. 3) Three-dimensional images can be re-orientated easily by changing the rotational axis. 4) Internal structures can be visualized by slicing the images at coronal, sagittal, and axial views. 5) Various anatomic structures can be observed independently, such as teeth and bones.
While new methods have been introduced to analyze 3D CBCT images, they may be complicated to understand and implement. Further, there have been many studies reporting linear measurements from A point, B-point, and Pog to the NTVL derived from 2D lateral cephalograms. To date however, no studies have reported analogous measurements derived from 3D CBCT images.
Therefore, the aims of this study were to investigate a simple method for assessing anterior-posterior jaw relationships via 3D CBCT images taken in the NHP relative to the nasion true vertical plane (NTVP), and measure normative data in Korean adults with normal profiles.
MATERIALS AND METHODS
The protocol of this study was reviewed and approved by the Kangnam Sacred Heart Hospital Institutional Review Board (2013-06-48), and written informed consent was obtained from all subjects. The subjects were selected from patients presenting for third molar extraction and evaluated as having normal profiles by three examiners (one orthodontist, one oral-maxillofacial surgeon, and one general practitioner).17 Inclusion criteria for subjects with a normal profile were skeletal Class I (A-point Nasion B-point [ANB] angle, 2° to 4°), Angle classification Class I, and full permanent dentition stage. CBCT images were converted to lateral cephalometric images via In Vivo Dental software (version 5.3; Anatomage Co., San Jose, CA, USA), to measure ANB angles. Exclusion criteria included a history of orthodontic treatment, orthognathic surgery, and prosthetic treatment of more than 3-unit bridges. Subjects with more than two missing teeth were also excluded.
Facial profile photographs were taken with the subjects sitting down in front of a mirror (Figure 1A) with their feet apart corresponding to the width of their shoulders, and their arms relaxed. Subjects were asked to stare at their own eyes in a 30 × 40-cm mirror after exercising their head up and down. Subjects were positioned 150 cm from the mirror. A plastic chain was hung on the background wall to serve as a plumb reference line. The camera (Nikon D80; Nikon, Tokyo, Japan) was set at the appropriate focal distance from the subjects.
CBCT images were also taken sitting in the NHP according to Solow and Tallgren's method (Figure 1B).18 The subjects were asked to sit in the chair of the CBCT machine with their feet apart corresponding to the width of their shoulders, and their arms relaxed. They wore eyeglasses fitted with a fluid leveler to verify changes in head posture during image scanning. As above, subjects were asked to stare at their own eyes in a mirror after exercising their head up and down. A 40 × 50-cm mirror was hung on the wall 1.5 m from the subjects. Subjects' heads were positioned without a chin support or any other type of headholder. Full field of view (23 × 17 cm) images were taken with a CBCT scanning machine (KaVo Dental GmbH, Biberach, Germany) with operational parameters of 120 Kv, 37.1 mA, a voxel size of 0.3 mm, and a scan time of 8.9 seconds. CBCT data were saved in Digital Imaging and Communications in Medicine (DICOM) format and the data were rendered and analyzed with In Vivo Dental software.
The angle formed between Ricketts' E-line and the true vertical line (TVL) derived from the plumb plastic chain in the facial profile (Figure 2A) was measured. Similarly, the angle between the E-line and the NTVP in CBCT images (Figure 2B) was measured. Subjects with 2° of difference or less between the two angles were selected. The resultant group was comprised of 80 subjects, 39 males with an age range of 18–45 years and a mean age of 27.6 years, and 41 females with an age range of 18–45 years and a mean age of 29.4 years.
The process of constructing the NTVP was achieved as follows, using In Vivo Dental software. First, the entire volumetric field of view represented as a square box was visualized on the volume rendering screen with high brightness. The operator digitized three points on the bottom surface after the square box was appropriately positioned (Figure 3). The bottom surface of the box was later used as a parallel plane to the true horizontal plane (THP) passing through nasion. Second, the midsagittal plane was constructed perpendicular to the line connecting box1 and box2 points and passing through nasion. Finally, after the THP and midsagittal plane were constructed, the NTVP was constructed via a coordinate system which was perpendicular to the two planes and passing through nasion (Figure 4). The linear measurements of A-point, B-point, and Pog were generated by the software after digitizing all landmarks (Figure 5). Student's t-test was used to assess sexual differences between these measurements. Statistical analyses were performed with Statistical Package for the Social Sciences software (version 12.0; SPSS Inc., Chicago, IL, USA).
RESULTS
Digitizing method error was assessed via 20 subjects selected randomly, where one observer digitized each subject twice at 1-week intervals. Dahlberg's formula was used to assess intra-observer reproducibility.19

(RE, random error; d, difference between the two measurements; n, number of subjects)
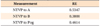
Digitizing method errors were 0.53 mm for the NTVP to A-point, 0.38 mm for the NTVP to B-point, and 0.46 mm from the NTVP to Pog (Table 1).
The respective mean linear measurements of A-point, B-point, and Pog relative to the NTVP were 0.18 mm (standard deviation [SD] 4.77 mm), –4.00 mm (SD, 6.62mm), and –2.49 mm (SD, 7.14 mm) in Korean males, and 1.48 mm (SD, 4.21 mm), –4.07 mm (SD, 6.70 mm) and –2.91 mm (SD, 7.25 mm) in Korean females. There were no statistically significant differences between Korean males and females (p < 0.05) (Table 2). Table 3 shows a comparison of the linear measurements obtained in this study and the results of other studies.1011
DISCUSSION
Facial profile is critically important when orthodontists and oral surgeons perform cephalometric analysis and treatment planning of patients. Intracranial references such as the SN line and FH plane have their shortcomings and do not always reliably reflect facial profiles, potentially leading to misunderstandings and patient dissatisfaction. There are two main reasons why this may occur. First, clinicians can only recognize whether or not intracranial references coincide with a patient's profile after a cephalogram or a CBCT image is obtained. Second, inter-individual variation in intracranial references is so broad that they often cannot be utilized reproducibly. Madsen et al.20 showed that the standard deviation of the angle between the THP and the FH plane was 4.6° in 57 subjects with an age range of 12–18 years, and the reproducibility of the NHP was only 2.1°. Bjerin6 also reported that the angle between the FH plane and THP exhibited substantial variation, ranging from –13.8° to 13.0°. Lundström et al.8 suggested that the angles between the SN line and THP were 3.8° (SD, 5.3°) in 27 boys and 4.1° (SD, 5.0°) in 25 girls. Further, if the SN to THL angle of a patient is large, a skeletal Class I relationship could be misinterpreted as a skeletal Class III relationship.6 Thus, cephalometric measurements using intracranial references cannot reliably reflect facial profile, and may be responsible for unexpected treatment results. Therefore, there is a strong need for references that reflect a patient's facial profile with minimal errors.
The reference system utilizing the NHP as an alternative to intracranial references has been studied since the late 1950s. The most important factors of the NHP are intra-individual reproducibility and reliability. Solow and Tallgren18 showed that the method errors of angles formed between the SN line and TVL, SN line and odontoid process tangent (OPT), and OPT and THL were 1.43°, 1.43°, and 1.95° respectively. Moreover, Moorrees and Kean7 reported that the variation of the NHP was 1.3° to 2.0°. Lundström and Lundström5 showed 1.5° to 2.0° variation. Weber et al.21 also showed that the NHP had high reproducibility in 3D space with a 3D camera system and a CBCT scanning machine. Therefore, extracranial references based on the NHP may be more appropriate for orthodontic diagnosis than intracranial references.
In 1999, Arnett et al.22 suggested the TVL in the NHP passing through subnasale as an orthognathic surgical guideline. It is thought that the TVL is not an appropriate reference line for orthognathic surgical design because the subnasale itself can shift to another position during two-jaw surgery. In 1990, Michiels and Tourne10 used the NTVL based on the NHP as a fixed reference passing through nasion. The anterior-posterior relationships of the maxilla and mandible were evaluated by calculating the perpendicular distance from A-point, B-point, and Pog relative to the NTVL.
There are many advantages of using the NTVL for diagnosis and treatment planning: 1) Patients easily and intuitively understand the resulting sagittal skeletal relationships because clinicians can express them in mm units. 2) Orthodontists can communicate with oral surgeons with regard to orthognathic surgical patients in terms of linear measurements relative to the NTVL. 3) The satisfaction of patients may be improved because treatment planning reflects the facial profile using the NTVL. Michiels and Tourne10 have asserted that the linear measurements between the A-point and B-point and the NTVL are more accurate than angular measurements such as the SNA, SNB, and ANB for classifying retrognathic, orthognathic, and prognathic profiles. They showed that the linear measurements of A-point and B-point relative to the NTVL were not correlated with facial profile independently, and the horizontal distance from A-point and B-point to the NTVP was highly correlated with it.
We need normative linear measurements to apply this concept to orthodontic diagnosis and treatment planning. Michiels and Tourne10 have reported the perpendicular distances from A-point, B-point, and Pog to the NTVL in 27 female Caucasians with normal profiles. Leitão and Nanda11 also measured the same parameters in 284 male Caucasians. These studies were performed with conventional lateral cephalograms, and were thus subject to the many errors associated with this methodology, including projection and identification errors.23 Although compensation of errors in the conventional cephalogram images was attempted, the resulting accuracy was less than that of CBCT images. Given these limitations, it is advantageous to use CBCT images for more accurate diagnosis, treatment planning, and evaluation after treatment.
The results of this current study (Table 2) were compared with those of Michiels and Tourne's10 and Leitão and Nanda's11 study (Table 3) to compare the normal facial tendencies of different races, although their data were derived from conventional lateral cephalograms. The anterior-posterior position of the maxilla of Korean male adults was similar to that of Caucasian male adults. However, the mandibular position of Korean adults was further forward than that of Caucasian males. Both the maxilla and mandible were more protruded in Korean female adults than in Caucasian female adults. The horizontal differences in A-point and B-point were higher in Korean females. These results show that Korean females have more of a skeletal Class II tendency than Caucasian females.
Most 3D CBCT scans are subject to a degree of motion artifacts because the orientation of the patient's head can move slightly during acquisition.24 It is often advisable to use a head strap to fix the patients head, to reduce motion artifacts. However, if a head restraint device is used, it may position the patient's head in a non-physiological position. Several studies have investigated the reproducibility of the NHP in 3D CBCT.21 Many methods have been introduced to determine the 3D NHP of patients reproducibly. Damstra et al.24 placed markers directly on the patient's face. Soncul and Bamber25 used a calibrated laser surface scanner to capture the 3D geometry of the patients' face. Xia et al.26 utilized a device consisting of a digital sensor attached via an individual bite jig. A facebow equipped with a spirit level27 and stereophotogrammetry28 have also been used to obtain repeatable head posture.
In this current study, two fluid levelers were attached at the front and lateral side of the frame of a pair of eyeglasses. Each fluid leveler was designed to turn easily so that the operator could adjust it horizontally regardless of the position of the eyeglasses. The fluid levelers were useful for verifying head movements during CBCT scanning.29 If the air bubble in the fluid leveler moves to one side during scanning, it means significant head movement occurred in the coronal or sagittal planes. In these situations, the patient's head position may be corrected before taking the CBCT image or, less commonly, the image can be retaken.
The human body demonstrates physiologic process and reflexes that allow reproducible 3D head posture. According to Weber et al.,21 physiological head position in the coronal plane is controlled by the vestibuleocular and vestibule-spinal reflexes, as well as inner ear otolithic gravitation. Head position in the axial plane largely depends on the vestibular balance system, and is supported by muscle balance and visual input.30 Head position stability in the sagittal plane depends on the memory system.30 People with habits such as working non-ergonomically on a computer or using a cellular phone for long periods of time often exhibit a downward position of the head and a habitually unbalanced head position.31 Therefore, there is a need to obtain a relaxed head position by performing stretching and neck exercises before taking CBCT images.
Weber et al.21 also reported statistically significant differences between three reference planes, with the coronal plane exhibiting the least variation overtime, followed by the axial plane then the sagittal plane. Of the three planes, head posture in the sagittal plane exhibited the largest variation. In this current study, the angle formed between Ricketts' E-line and the TVL derived from the plumb plastic chain was measured in facial profiles (Figure 2A), and the angle between the E-line and the NTVP was measured in CBCT images (Figure 2B) to verify movements of head posture in the sagittal plane.
A new reference plane, the NTVP, was used in this study to assess anterior-posterior jaw relationships. The linear norms from A-point, B-point, and Pog to the NTVP may be used as a useful guideline for orthodontic tooth movements and orthognathic surgical movements in the sagittal plane. Notably, it is thought that the sample sizes in this study are not sufficient for determining definitive normative parameters of the linear measurements investigated. Therefore, further research with larger samples and incorporating several cephalometric variables such as the effects of incisor position and inclination on facial profiles is needed.
CONCLUSION
The NTVP based on the NHP can be constructed on CBCT images using a square box plane, and used to measure the linear distances from it to the maxilla and mandible. Three-dimensional analysis of CBCT images using the NTVP is a simple and reliable method for assessing anterior-posterior skeletal relationships.






 XML Download
XML Download