

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The stability of the outcome of orthodontic treatment is a major clinical concern, as retraction of periodontal fibers might cause many cases to eventually relapse, particularly after alignment of the anterior teeth of the mandible.12 Many clinicians consider permanent or long-term retention to be the only way to maintain a proper post-treatment alignment.23 One method for maintaining long-term retention is to use fixed retainers that remain permanently in the mouth and are invisible, well tolerated, and do not require patient compliance after application by an orthodontist.24 Nevertheless, approximately 10% to 47% of fixed retainers fail because of wire fractures or bond failures.2456
Previously, fixed retainers were fabricated from thick stainless steel round wires and were later made from thinner coaxial or braided round wires.245 Recently, fiber-reinforced composite (FRC) resins were introduced as an alternative to stainless steel archwires to reduce the bulk of the lingual retainer.2789 FRC retainers are flexible and able to easily conform to tooth surfaces. Additionally, they are esthetically accepted, nickel-free, biocompatible, and easily repairable.210111213 However, the main disadvantage is that FRC retainers produce a rigid splint that limits physiological tooth movement and may contribute to a higher failure rate.26
The development of a method for long-term retention is important for treatment stability and to prevent further problems, such as incisor crowding.21415 The most appropriate method for assessing retainer success is to perform a long-term randomized clinical trial. However, only a limited number of studies have been conducted to assess FRC retainers,2131617 and few studies have extended longer than 1 year.18 Furthermore, the results of previous studies do not favor any specific method, and there is no consensus on which method is the best.192021
Both conventional wire retainers and FRC splints have specific disadvantages. Conventional retainers are made of active orthodontic wires and are thus rather technique-sensitive and time-consuming to position passively on the lingual surface. Additionally, these types of retainers can either debond or exert undesirable orthodontic forces on aligned teeth. FRC splints are expensive and even more technique-sensitive than conventional retainers. They may have higher failure rates, they are more difficult to repair, and they may cause additional periodontal conditions.26172223 Therefore, a more flexible yet strong wire design might be advantageous over the abovementioned types in terms of passivity (i.e., theability to conform to the patient's dentition without exerting orthodontic force), the likeliness of debonding, cost, and chairside time. We hypothesize that a retainer composed of twisted ligature wire might provide these advantages.
This 2-year prospective preliminary randomized clinical trial was conducted to compare the success rate of an experimental dead soft twisted wire (TW) retainer, which has not been assessed previously, with FRC and flexible spiral wire (FSW) retainers. The null hypothesis was that there would be no difference in the success rate between the three retainer types. Success was defined as the lack of any failure, ranging from a single-tooth debond to a total retainer breakage.
MATERIALS AND METHODS
This explorative, prospective preliminary single-blind randomized clinical trial originally enrolled 150 (50 × 3) fixed orthodontic patients who were monitored over 2 years. The sample size was predetermined as n = 40 × 3 based on previous clinical research on retainers. To compensate for potential dropouts during the study period, three groups of 50 patients each were initially recruited.
Ethical considerations and potential harms
The study protocol was approved by the research committee of the research department of the university, in accordance with the Helsinki Declaration (ethical approval #2318). All patients (or their parents) were verbally informed of the purpose of the study, and they all signed routine informed consent forms. The subjects could request to change or remove the retainer (and leave the study) at any time during the study. No adverse events were identified during the study.
Subject screening and eligibility criteria
Patient recruitment was carried out in 2012 and 2013. The selected patients had been previously treated in a private office with standard MBT 0.022-inch (in) slot fixed appliances. The subjects were sequentially included based on the criteria described below and randomly assigned to one of the groups until each group reached 50 patients.
We included healthy participants who provided consent and had no history of previous dental extraction or orthognathic surgery, with an original indication for non-extraction treatment (Class I crowding, incisor mandibular plane angle [IMPA] < 92°, vertically normal or horizontal and no pattern of vertical excess, and with a crowding extent and soft tissue characteristics appropriate for non-extraction treatment). After the treatment period, patients were included if they had ideally aligned dentition, a Class I relationship with an overbite/overjet between 1 and 3 mm, no issues contraindicating or interfering with retention, clinical signs suggesting bruxism or clenching, advanced dental abrasion/attrition/erosion, and a need for mandibular canine-to-canine fixed retention. We included patients who had good oral hygiene, healthy periodontal condition, and no previous history of using bonded retainers. The probing pocket depth was assessed and radiological examinations were performed to detect any periodontal problems. Patients with widespread probing depths more than 3 mm and radiographic evidence of periodontal bone loss were excluded.
Randomization and blinding
Random allocation was accomplished by the same orthodontist who enrolled the participants using a random number table. The study was single-blind: Each patient had layperson knowledge of his/her own retainer, but he/she had no knowledge (either technically or in layperson terms) of the other designs involved in the study.
Interventions
The experiments were performed using lingual canine-to-canine retainers, all bonded in a similar fashion, as described previously.2224
Retainer types
In the first group, 0.0175-in FSW (Ortosmail; Krugg Spa, Milan, Italy) was used. In the second group, an FRC splint (Everstick Ortho; Stick Tech, Turku, Finland) was used. In the third group, as described here for the first time, the retainers were fabricated by a left-handed orthodontist by carefully twisting two 0.009-in dead soft wires (Ligature wire; 3M Unitek, Monrovia, CA, USA) using a Mathieu plier to form a passive yet sufficiently strong bundle. The extent to which the wires were twisted (the number of twists per millimeter of wire) was similar between all specimens. The wires were twisted clockwise, 6 rounds per 10 mm. The bundle was formed against the lingual surface of the anterior teeth on a dental plaster.
Uniform bonding protocols
After scaling and polishing (using fluoride-free pumice) the lingual surface of the mandibular anterior teeth, full isolation was carried out using cheek retractors and cotton rolls in the labial and lingual areas. The surfaces were etched with 37% phosphoric acid (3M Unitek) for 40 seconds followed by 30 seconds of rinsing and then thorough air-drying with an oil-fee syringe. Two layers of light-curable primer (Ormco, Orange, CA, USA) were added to the surface. Each layer was light-cured for 20 seconds (Optilux 501; Kerr Corp., Orange, CA, USA; light intensity, 930 mW/cm2; wavelength range, 400-505 nm). The retainers were prepared and contoured on plaster casts.
A layer of resin (Transbond XT; 3M Unitek) was applied after placement to stabilize the retainer on the lingual surface, followed by light-curing for 20 seconds. Afterwards, a layer of restorative composite (Z100; 3M Unitek) was placed over the retainer and light-cured for 40 seconds. Finally, excess resin was removed from the interproximal areas using a scaler, and the restorations were polished.2224 Each patient was instructed not to bite on hard or sticky foods with the anterior teeth to avoid disruption of the bonded retainers. The patients were thoroughly advised on this issue at the end of each visit.
Follow-up and retainer failure
Each patient was followed up once a month for 2 years or until the failure of the retainer. Retainer failure was defined as the first detachment of any composite pad or breakage/distortion of the retainer. Debonded retainers were routinely re-bonded or replaced depending on the severity of the case. The failure time was recorded for the survival analysis.
If a patient missed a follow-up session and visited the next month with an intact retainer, he/she remained in the study. However, if the retainer had failed during any period of absence lasting more than a month, the patient was excluded. Patients who stopped attending the follow-up sessions were excluded. The exclusion of a patient or the failure of a retainer did result in the discontinuation of treatment, as the patients continued to receive routine healthcare.
Statistical analysis
Descriptive statistics were calculated for each group. The ages were compared using an analysis of variance (ANOVA). The gender distributions were compared using a chi-squared test. The failure rates of the three groups of retainers were calculated using a Kaplan-Meier estimate and compared using a chi-squared test and a Cox proportional hazard regression using IBM SPSS Statistics ver. 20.0 (IBM Co., Armonk, NY, USA). The level of significance was set at 0.05.
RESULTS
More than 180 patients were assessed until 50 × 3 patients were included. Of the 150 enrolled patients, 22 were removed from the study because of failure to regularly attend the follow-up sessions. Finally, 42, 41, and 45 patients who received an FRC splint, an FSW retainer, or an experimental TDW retainer, respectively, were included in the analysis. The trial ended after 24 months of follow-up.
The mean age of the included patients was 18.0 ± 3.6 years (range, 13–25 years). The average ages were 18.5 ± 3.6, 18.4 ± 3.7, and 17.0 ± 3.4 years, respectively, in the FRC, spiral flex, and TDW groups. The average ages were similar between the three groups, according to the ANOVA (p = 0.102). The FRC splint was used for 23 men and 19 women, the FSW retainer was used for 17 men and 24 women, and the TW retainer was used for 20 men and 25 women. The difference between the gender distributions of the groups was not significant (chi-squared p = 0.441).
Failure rates
All of the detachments occurred at the enamel junction. Of the FRC, FSW retainer, and TDW retainers, 15 (35.7%), 11 (26.8%), and 8 (17.8%) failed, respectively. Three FRC retainers, one FSW retainer, and one TW retainer broke during the stud period, and the rest of the failures were caused by detachment. The chi-squared test failed to detect a significant difference in the failure rates between the groups (p = 0.167, Table 1).
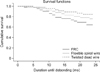
Duration of successful retainer use
The average duration of success was approximately 21 months, according to the Kaplan-Meier estimates (Table 1). The Cox regression analysis showed no significant overall difference between the treatments (p = 0.146, Figure 1, Table 2), although a marginally significant difference was detected in the survival rates between the FRC and TDW retainers. A hazard ratio of 2.3 indicated that the risk of failure may be two times higher in the case of FRC retainers compared to TDW retainers, with a non-statistical trend (p = 0.057, Table 2). The risk of failure was approximately 50% less for TDW retainers compared to FSW retainers, though it was not statistically significant (p = 0.317).
DISCUSSION
We did not observe an overall statistically significant difference between the success rates of the three retainer types. Nonetheless, the experimental retainers showed better survival results compared to the FRC retainers. Similar to metallic alloys, fibers might offer superior mechanical properties, while composite resins provide esthetic benefits.6222526 Considering the increasing number of adult patients seeking orthodontic treatment, esthetics is now a major factor contributing to patient satisfaction.2227
FRC retainers have advantages, including biocom patibility (no metal content), making them safe for patients who are allergic to metals or who are undergoing MRI assessments, and FRC retainers can be bonded to dental tissues.2228 FRCs have been intro duced in dental practice in recent years. The possibility of reinforcing composite resins with fibers such as aramid, polyethylene, carbon, or glass has numerous clinical applications, including the replacement of missing teeth, repair of complete dentures, preparation of overdenture parts, splinting of periodontal teeth, use in Maryland Bridges, or the direct construction of posts and cores.132229 The flexural strength of FRCs might be similar to that of gold and Cr-Co alloys and greater than that of stainless steel.222530 In orthodontic treatment, FRCs have passive and active applications, such as post-orthodontic tooth retention and anchorage unit increases.62226 Glass FRCs are recommended for post-orthodontic fixed lingual retention in the anterior segment.6222526 The clinical efficacy of FRC retainers may be based on the internal structure of the complex. The resin of the matrix and the adhesive system integrate with fibers. The homogeneous structure of integrated resin matrix, adhesive, and fiber might absorb and dissipate mechanical stresses.622252630 Conventional retainers use mechanical retention between non-bondable materials, such as metal and composite adhesives, creating a point of weakness at the junction between different materials.6222526 Multistranded FSWs are broadly accepted for routine use in modern orthodontics.6172226
Both FRCs and multi-stranded wires used for postorthodontic retention have shown 2-year success rates of approximately 50% to 90%.17222830 In this regard, our findings are consistent with studies reporting better results with multi-stranded wires compared to FRC retainers, such as polyethylene ribbon-reinforced or glass fiber-reinforced (GFR) retainers, in vivo1317 or in vitro.16 For instance, the average success durations were approximately 24 and 12 months for multi-stranded and FRC retainers, respectively.13 Another study showed significantly higher success rates for multi-stranded retainers (88%) compared to GFR retainers (49%).17 FRC retainers might have a higher failure rate because of their lower flexibility, which results in higher strain in the inter-dental areas under loading.231 This can lead to a higher probability of microfracture or debonding, particularly in the case of teeth that have become more mobile after orthodontic treatment.213173132 Other chemomechanical properties, such as water sorption and thermal expansion of polyethylene materials, might also contribute to the higher failure rates of FRC retainers.213 Capillary forces might cause water to enter non-polymerized voids along the woven fibers and alter the mechanical characteristics.213 Moreover, the lingual placement of FRC, which is necessary for esthetic reasons, is not the best option to reinforce a composite.17333435 Furthermore, FRC retainers are technique-sensitive, which may indicate higher rate of human error.17 Multi-stranded retainers have suitable efficacy and reliability; hence, they are considered a standard treatment option in modern orthodontics.245 Despite the success of multi-stranded retainers, splinting the teeth with an FRC is also a popular choice.212 On the other hand, the results of the present study are in contrast to some previous studies showing insignificant differences between multi-stranded metal wires and FRC retainers.22228 The discrepancies might be attributable to the use of different materials and methodologies, including differences in the method used for light curing (light-emitting diode versus quartz-tungsten halogen), which might affect the polymerization, or differences in the interval for follow-up (6-month follow-up visits versus monthly follow-up visits).22
This study was limited by several factors. It would be preferable to include more specimens (based on power calculations) and to evaluate other FRC designs and maxillary retainers for a longer duration. The insufficient sample size makes this study inconclusive. In addition, if the sample size were increased, a p-value less than 0.05 might be obtained in the comparison between FRC and TDW, which resulted in a p-value of 0.057 in this study. It should be noted, however, that conducting a 2-year pilot study for a retainer type that has not been previously investigated could postpone such a project for another 2 or 3 years. Therefore, the authors decided to conduct this trial without a pilot study. Moreover, although we considered numerous inclusion/exclusion criteria to ensure a uniform sample, the control of patient factors was lacking. It would be preferable to also control for chewing habits, vertical skeletal patterns, and inclination of the lower incisors, which might influence the success rate.
This study was advantageous in terms of the use of standardized materials for bonding,22 the well-balanced groups and homogenous randomization of the treatments,17 and the introduction of a successful retainer, which might be more flexible than the traditional spiral wires. Nevertheless, the mechanical properties of this new retainer should be assessed and optimized in follow-up in vitro studies. Moreover, although the orthodontist made efforts to exert a similar force while twisting the dead wires, it was impossible to standardize this factor without the use of automatic machinery. Still, the wires were twisted the same number of times per unit of length. The generalizability of this study is improved due to the recruitment of subjects of both genders and of different ages. However, the findings are only generalizable to the mandible and to the material brands used (results achieved with a particular brand are less likely to be generalizable to other brands). Future studies should also evaluate the gingival response to the experimental retainer.
CONCLUSION
Within the limitations of this preliminary clinical trial, the three types of retainers, including the experimental retainer created by twisting two dead soft wires, appear to present similar success rates within a 2-year follow-up period. The survival rate of the experimental TW retainers might be better than that of the FRC retainers, although we cannot decisively conclude this from a statistical point of view, and future studies with larger samples are necessary to confirm or reject the success of this retainer and to assess the gingival response. Although the superiority of the TDW retainer over the FRC could not be confirmed, the results show that the TW retainer was at least equivalent to the FRC.


 XML Download
XML Download