

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
When a controlled and predetermined force is delivered onto a tooth during orthodontic treatment, the alveolar bone on the tension side exhibits a proliferative response, while the pressure side shows a resorptive response. A series of mechanical, physical, and biochemical processes are involved in moving a tooth, or set of teeth, to an aesthetically and functionally desirable location. Detailed assessment of the height and width of the alveolar bone is necessary to induce controlled three-dimensional (3D) movement of the tooth. Therefore, the alveolar bone metrics are an important consideration during orthodontic treatment.
The premolars, similar to other teeth, are critical for efficient mastication as they bear occlusal forces and are important in maintaining the vertical dimension of the face morphology. Thus, premolars contribute to both function and maxillofacial aesthetics. The facial growth pattern is established at an early age prior to the eruption of the maxillary first molars. The vertical facial type is an important indicator of maxillofacial harmony during facial growth and is divided into long face, normal face, and short face types based on the Frankfort mandibular angle (FMA). Vertical facial type and orthodontic treatment are interrelated, and the alveolar bone, muscle, and malocclusion differ considerably according to the vertical facial type, which can influence therapeutic planning.1 Vertical facial type is an indicator of craniofacial growth2 and thus influences the selected treatment and force applied during orthodontic treatment.
Tsunori et al.3 demonstrated that the thickness of the entire buccal cortical bone and lingual cortical bone in the first and second molar regions was greater in short faced individuals than in average and long faced individuals. The basal cortical bone thickness of the left central incisor section was also greater in short faced subjects. A study conducted by Gracco et al.4 on the position of the upper central incisors revealed that the alveolar bone thickness was greater in short face type patients than in long face patient types. In addition, the root apex of the upper incisors was further from the lingual cortex in short face type and norm face type patients than in long face type patients. Yamada et al.5 showed that the distance between the central incisor apex and the inner contour of the labial cortical plate was significantly shorter than the distance to the lingual cortical plate. Handelman6 delineated the limits of orthodontic treatment in mature adults, which are important when making treatment decisions. The labial and lingual cortical plates at the level of the incisor apex may represent the anatomic limits of tooth movement. Orthodontic tooth movement may be limited in patients with narrow alveolar bone widths, and these patients are likely to experience increased iatrogenic sequelae, such as bone loss, root resorption, and gingival recession. Masumoto et al.7 revealed that the cortical bone of the first and second molar sections was thicker in short faced subjects than in average and long faced subjects. These results are evidence of the significant and complex relationship that exists between the mandibular structures and facial type. The morphological features related to masticatory function and facial types are associated with the cortical bone thickness of the mandibular body.
In the past decade, cone-beam computed tomography (CBCT) devices have been developed for head and neck imaging. These dedicated maxillofacial diagnostic devices reduce cost and the radiation dose to patients, and are well suited for imaging the craniofacial area,8 resulting in improved treatment planning. CBCT generates images with high spatial resolution, both longitudinally and axially, by applying an isotropic voxel matrix to the dento-maxillofacial region.9 CBCT has been used to determine the positioFn of teeth relative to anatomical landmarks.4
The aim of this study was to compare the positions of the mandibular premolars using CBCT between Angle Class I patients with different vertical facial types. The CBCT parameters were measured and analyzed in order to detect any differences in the mandibular premolar positions in Class I patients with different facial types. The findings could serve as a reference enabling more effective orthodontic planning and improve the control of forces during tooth movement.
MATERIALS AND METHODS
Subjects
A total of 120 Angle Class I patients aged 18-40 years who received routine orthodontic treatment at the Affiliated Hospital for Stomatology, Chongqing Medical University (Chongqing, China) were randomly chosen for this study. Patients were included in the study based on their FMA values and were divided into three 40-subject groups as follows: short face type (FMA < 22°), norm face type (22° ≤ FMA ≤ 32°), and long face type (FMA > 32°).10 The study was approved by the Research and Ethics Committee of the Affiliated Hospital for Stomatology, Chongqing Medical University. The subjects were informed of the study and provided written informed consent to participate.
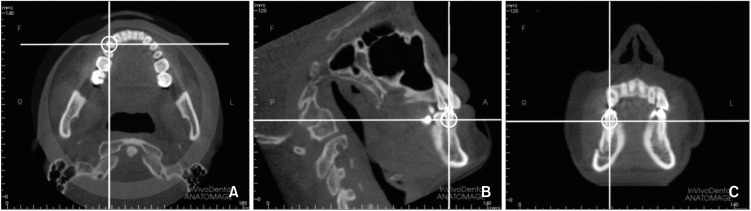
The anatomic parameters were measured using CBCT, and the images were reconstructed using InvivoDental 5.1 software (Anatomage, San Jose, CA, USA). The CBCT device (Classic i-CAT CBCT; Imaging Sciences International, Hatfield, PA, USA; Figure 1) was set at 120 kV and 5 mA. Images were captured at a single 360°-rotation over 8.9-seconds and digitized using InvivoDental 5.1 software for analysis. During image acquisition, the head of each subject was oriented with the midsagittal plane perpendicular to the floor, and the subjects were instructed to bite in centric occlusion during exposure. All landmarks were identified and measured using the same software.
Inclusion criteria
(1) All subjects were diagnosed with skeletal Class I and molar and canine Angle Class I, and were aged 18-40 years.
(2) All relevant information prior to treatment, including medical history, study models, cephalometry, and panoramic radiographs was completely available in all subjects.
(3) Subjects had permanent dentition in the premolar and molar regions without crowding. In addition, subjects did not have any dentition defects or edentulous spaces.
(4) The first and second premolars were single-rooted with complete root development.
(5) Periodontal tissue was healthy with no gingival recession and no horizontal or vertical absorption of the alveolar bone.
Exclusion criteria
Patients who received endodontic, prosthodontic, or orthodontic treatment; those with maxillofacial deformities or trauma; and those who underwent surgery of the stomatognathic system were not included in this study.
CBCT protocol
Image acquisition and reconstruction
The 120 subjects meeting the inclusion criteria underwent CBCT using the same machine at uniform scan settings and conditions. Digital Imaging and Communications in Medicine (DICOM) files were generated and imported into the InvivoDental 5.1 software for 3D reconstruction (Figure 1). The subjects were then classified as short face type (FMA < 22°), normal face type (22° ≤ FMA ≤ 32°), and long face type (FMA > 32°), with 40 subjects per group. The observing axis was positioned at the mandibular right premolar in the sagittal and cross-section planes. The observing axis in the sagittal plane was aligned to the tooth axis so that the sole plane passing through the tooth axis could be confirmed in the coronal plane. The best observation position was adjusted based on these settings. All parameters were measured in the coronal plane.
Measured parameters
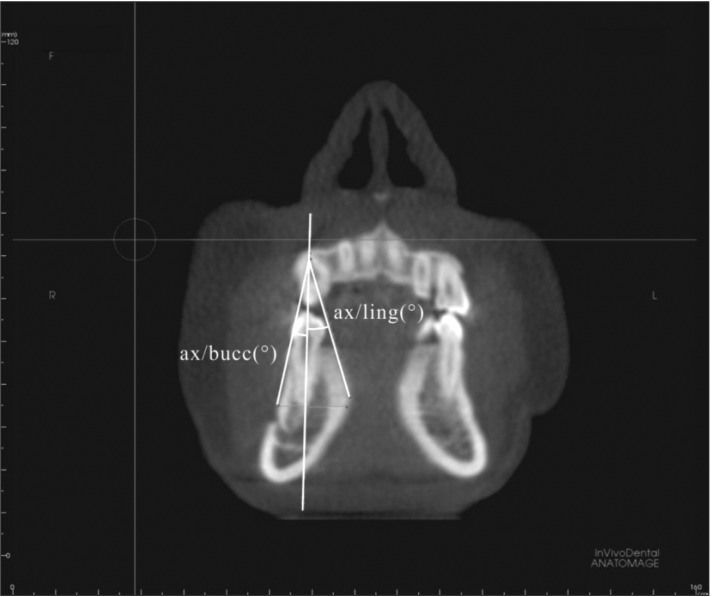
The relationship between the mandibular premolar and the mandible was determined by measuring the angle between the axis of the mandibular premolar and the buccal cortex, defined as the Premo ax/bucc cort (°), and measuring the angle between the axis of the mandibular premolar and the lingual cortex, defined as the Premo ax/ling cort (°), as shown in Figure 2.
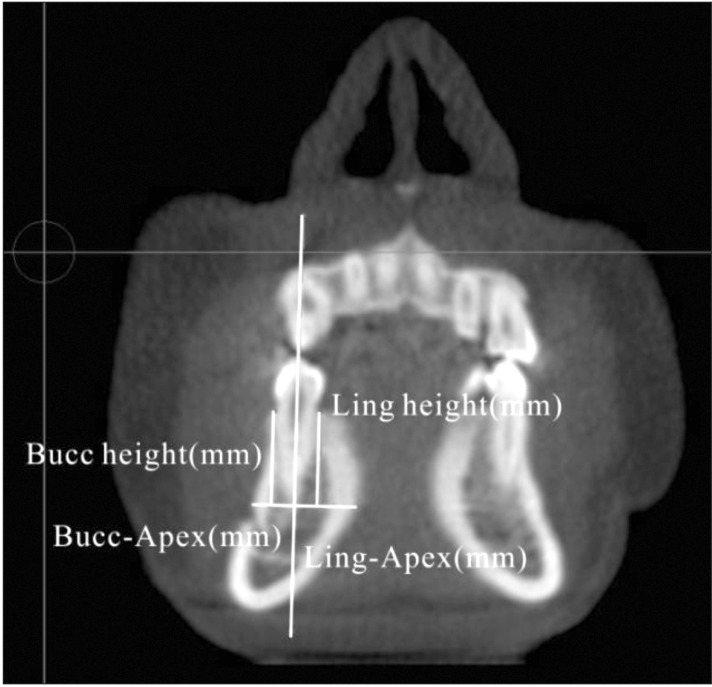
The alveolar bone thickness was determined by measuring the distance between the mandibular premolar root apex and the buccal cortical bone (Bucc cort-Apex [mm]) and measuring the distance between the mandibular premolar root apex and the lingual cortical bone (Ling cort-Apex [mm]), as shown in Figure 3. The measured distance was perpendicular to the axis of the premolar. The heights of the buccal and lingual alveolar bone (Bucc cort height [mm] and Ling cort height [mm], respectively) were measured as shown in Figure 3.
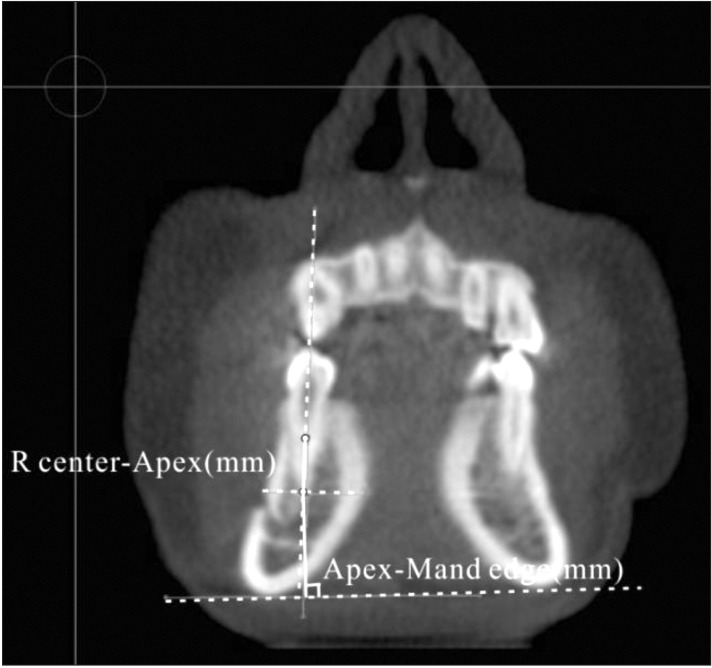
The distance from the resistance center of the mandibular premolar to its apex was measured. The resistance center was defined as two-fifths the distance between the alveolar crest and root apex (Resist center-Apex [mm]; Figure 4). The vertical distance from the mandibular premolar apex to the mandible edge (Apex-Mand edge [mm]) was determined as shown in Figure 4.
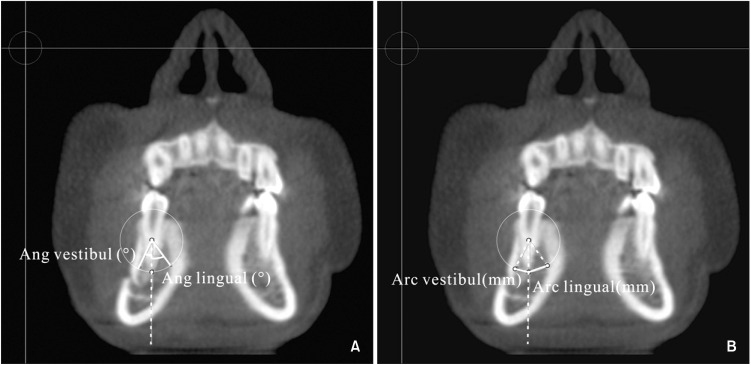
Parameters related to tooth movement range were determined by measuring the following: (i) angle of vestibularization in which one of the two sides corresponded to the distance between the center of resistance and the point at which the apex contacted the internal buccal cortex (Ang vestibul [°]; Figure 5A); (ii) angle of lingualization in which one of the two sides corresponded to the distance between the center of resistance and the point at which the apex contacted the internal lingual cortex (Ang lingual [°]; Figure 5A); (iii) arc of vestibularization, defined as the distance traveled by the apex until it contacted the internal buccal cortex during vestibularization, indicating the maximum possible inclination of the apex in the buccal direction without provoking resorption (Arc vestibul [mm]; Figure 5B); (iv) arc of lingualization, defined as the distance traveled by the apex until it contacted the internal lingual cortex during lingualization, indicating the maximum possible inclination of the apex in the lingual direction without provoking resorption (Arc lingual [mm]; Figure 5B); and (v) maximum possible movement, defined as the sum of the arcs of vestibularization and lingualization (Max poss movem [mm]; Figure 5B).
Statistical analysis
The mean and standard deviations (mean ± SD) were calculated for all measurements. The data were analyzed using SPSS statistical software ver. 17.0 (SPSS Inc., Chicago, IL, USA). The one-way analysis of variance (ANOVA) test was used for variance analysis among the facial type groups. The significance level was set at α = 0.05.
RESULTS
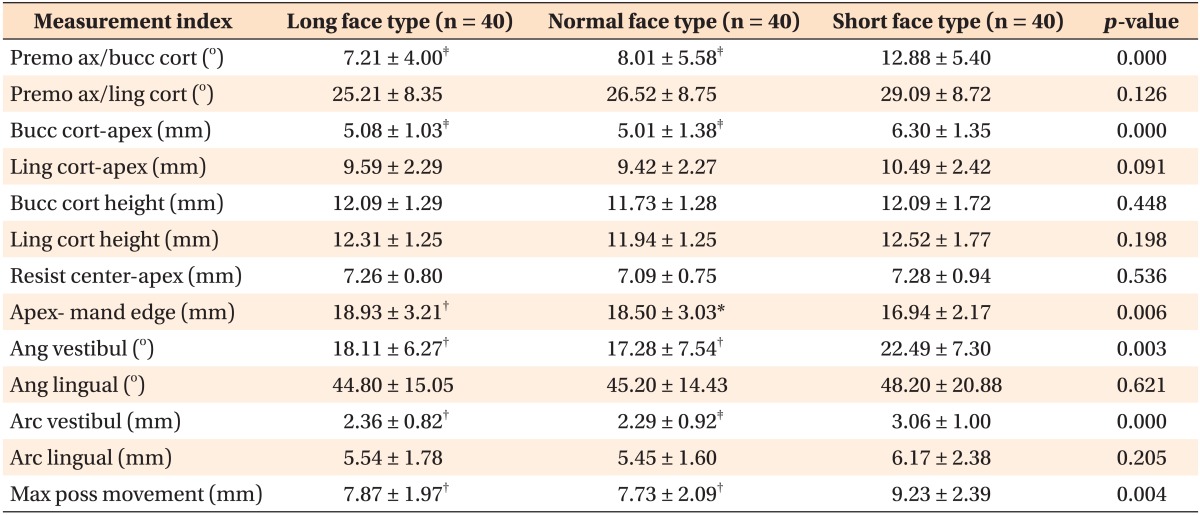
The various parameters were measured using CBCT to assess the position of the mandibular first and second premolars in 120 Class I subjects and compared between long, normal, and short face types (Tables 1 and 2).
As shown in Table 1, the following observations were made concerning the position of the mandibular first premolar in Class I subjects with different facial types. The angle between the tooth axis and buccal cortex differed significantly between the three vertical facial types (p < 0.01). The angle was significantly greater in short face types compared to both the normal (p < 0.001) and long face types (p < 0.001). The distance from the root apex to the buccal cortex and mandibular edge, the angle of vestibularization, the arc of vestibularization, and the root apex maximum movable distance differed significantly between the three vertical facial types (p < 0.01).
Except for the distance between the root apex and mandibular edge, these parameters were greatest in the short face type, followed by the long face type, and finally, the normal face type. The distance between the root apex and mandibular edge was significantly lower in the short face type compared to the long (p < 0.01) and norm face types (p < 0.05). The distance between the mandibular first premolar apex and lingual cortex was 1 to 2 times greater than the distance to the buccal cortex. The remaining parameters did not differ significantly (p > 0.05) between the three facial types.
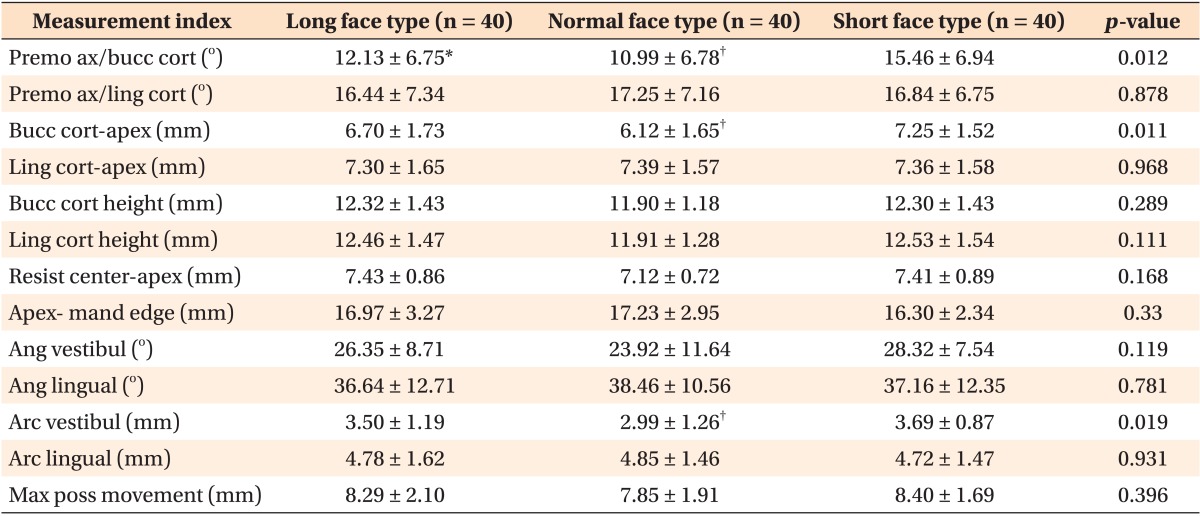
Table 2 summarizes the parameters indicating the position of the mandibular second premolar in Class I subjects with different facial types. The angle between the tooth axis and buccal cortex differed significantly between the three facial types and was greatest in the short face type, followed by the long face type, and the normal face type. The angle between the short face type and long face type differed significantly (p < 0.05), as did the short face type and normal face type (p < 0.01).
The distance between the root apex and buccal cortex differed significantly between the three facial types. The distance was significantly greater in the short face type than in the normal face type (p < 0.05). The arc of vestibularization also differed significantly different between the three facial types (p < 0.05), and was significantly greater in the short face type than in the normal face type (p < 0.01). The distance from the mandibular second premolar apex to the lingual cortex nearly equaled the distance between the root apex and buccal cortex in all facial types. For the remaining parameters, there were no significant differences between the three facial types.
DISCUSSION
Since the introduction of CBCT to general and specialty dentistry, its use has steadily increased in clinical orthodontics, implantology, temporomandibular joint imaging, and maxillofacial surgery due to its accuracy, resolution, and reliability. Numerous studies have shown the versatility and reliability of CBCT in cephalometric assessments. Timock et al.11 proved that CBCT could be used to quantitatively assess the buccal bone height and thickness with high precision and accuracy. Sherrard et al.12 showed that CBCT images were at least as accurate and reliable as periapical radiographs for determining the tooth- and root-lengths. Tarazona et al.13 similarly reported that CBCT digital models were as accurate and reliable as digital models generated from plaster casts. Ludlow et al.14 showed that the multi-planar reconstruction displays of CBCT volume images provided generally more precise identification of traditional cephalometric landmarks. Hassan et al.15 reported that measurements based on 3D-CBCT surface images were accurate, and small variations in the patient's head position did not influence the accuracy. Thus, CBCT has emerged as a promising technology with the potential to replace standard computed tomography as the method of choice for 3D-cephalometric analysis as it provides tomographic images and volumetric reconstructions at substantially less radiation and expense.
Thilander et al.16 showed that buccal alveolar bone dehiscence or fenestration can occur during labial tooth movement. Steiner et al.17 observed significant recession of the gingival margin, connective tissue level, and marginal bone when the incisors were moved approximately 3.05 mm labially in monkeys. Kaley and Phillips18 reported that during orthodontic treatment, the roots of impacted maxillary incisors in contact with the palatal cortical bone were at higher risk of resorption. In orthodontic treatment, the movable distance of the root apex is greater than the distance for the rest of the root. If the root moves past the cortical bone wall during orthodontic tooth movement, root or cortical bone resorption, dehiscence, gingival recession, and other adverse consequences may result. Therefore, the alveolar bone thickness should be considered during orthodontic treatment planning. In this study, we found that the buccal alveolar bone thickness in the mandibular first premolar was thicker in the short face type than in the long and normal face types. This suggests the importance of determining the movable distance for the mandibular premolars in patients with long and normal face types in order to prevent undue root or cortical bone resorption.
Edwards19 reported that the alveolar bone width in the incisor region is critical for orthodontic and orthognathic surgical treatment planning. Orthodontic treatment planning should consider the alveolar bone width, especially in cases where the bone is narrow or unable to accommodate a wide-range of tooth movement during orthodontic treatment, in order to avoid iatrogenic injury. Sarikaya et al.20 reported that the alveolar bone widths of the maxilla and mandible were significantly reduced after retracting the incisors, and some patients experienced bone fracture. Ten Hoeve and Mulie21 found that the teeth stopped moving if the root of the mandibular anterior teeth came into contact with the cortical bone during orthodontic treatment. Indiscriminate continuation of the force on the tooth in these situations would cause negative consequences, such as bone plate fracture and bone perforation at the labial-lingual side. The incisor periapical alveolar width is thought to limit the orthodontic tooth movement distance. Ten Hoeve and Mulie21 reported that in subjects undergoing orthodontic treatment using the Begg's technique, the incisors were forced into the alveolar bone prior to the movement of the teeth to the palatal side. This maneuver can increase the distance between the root apex and cortical bone plate, leading to entry of the apex into the wide alveolar area and preventing root injury that might otherwise occur due to undue contact between the root and cortical bone.
The classic Tweed-Merrifield technology attaches great importance to the three-dimensional direction of tooth movement (front, side, and rear) and vertical limits. These movements are considered important factors in orthodontic correction and in assessing recurrence. In this study, we show that the apical buccal removable space in the mandibular first premolar was larger in the short face type than in the long and norm face types. These observations suggest that application of torque to the mandibular first premolar in long and norm face types would increase the risk of the root contacting the buccal cortex, resulting in adverse consequences. The apical buccal removable space of the mandibular second premolar was larger in the short face type than in the normal face type. The rotation range of the root apex should therefore be assessed during treatment planning. Andrews22 asserted that the apex of the tooth axis after orthodontic treatment should be located in the middle of the alveolar bone in the bucco-lingual direction. In this study, the angle between the mandibular premolar tooth axis and buccal cortex, and the distance from the apex to the buccal cortex differed significantly between the three vertical facial types. Based on the measurements, the distance between the mandibular first premolar apex and lingual cortex was 1 to 2 times longer than the distance between the apex and buccal cortex. The second premolar apex pointed in the buccal direction and was positioned in the middle of the alveolar bone. Observations from this study differ from those reported by Andrews. This discrepancy may be due to the difference in the sample types selected for each study; the sample population in the current study comprised Class I subjects, whereas subjects in the Andrews's study22 were normal and did not have malocclusion. Our study suggests that the range in root movement was minimal in the long and normal face types in the buccal direction. Thus, adverse consequences, such as root resorption and bone fracture, can easily occur in Class I subjects with long and normal face types. It is important to note that certain vertical facial types are reportedly prone to root resorption; short face type patients are more susceptible to severe root resorption.23 The current study showed that the distance from the apex of the mandibular premolars to the buccal cortex was greater in short face types, which favors occlusal adjustment in the posterior tooth segment. However, a large magnitude of corrective force is required to move teeth in short face type patients due to the high strength of the masticatory muscle and the high bone density of the mandible. Excessive orthodontic force can result in root resorption24; therefore, this phenomenon must be prevented during treatment.
The lingual (palatal) side of the cortical bone height is one of the factors affecting the resistance center.25 Tanne et al.26 showed that root length and alveolar bone height influence the patterns of initial tooth displacements by altering the center of resistance, center of rotation, and magnitude of displacement. Anatomic variation in the root length and alveolar bone height should be considered when determining the forces to be delivered during orthodontic treatment in order to ensure optimal and desirable tooth movement. Choy et al.27 demonstrated that the location of the center of resistance changes significantly with variation in the shape and length of the root embedded within the alveolar bone. In contrast, the relative location of the center of resistance to the total root length remained constant in response to alveolar bone loss. Tapered and short roots were prone to tipping due to alveolar bone loss or apical root resorption.
It is critical to assess the height of the alveolar bone before beginning orthodontic treatment. Short face type patients require a greater force and more time during orthodontic tooth movement due to the high density of the mandibular bone and strong masticatory muscles in these patients.282930 However, excess force and duration can increase the risk of alveolar bone resorption. Hence, adequate data could be highly useful for achieving the desired treatment objective while avoiding complications. The results of this study showed that the alveolar bone height in the first and second premolar regions in the three vertical facial types did not differ significantly (p > 0.05).
CONCLUSION
1. In Class I subjects, the buccal alveolar bone thickness and root movable range in the buccal direction in the mandibular first premolars was greater in the short face type than in the long and normal face types.
2. In Class I subjects, the buccal alveolar bone thickness and root movable range in the buccal direction in the mandibular second premolars was greater in the short face type than in the normal face type; this trend was not observed for the long face type.
3. In this study, the distance between the mandibular first premolar apex and the lingual cortex was 1 to 2 times longer than the distance between the apex and buccal cortex. The second premolar apex was located along the buccal aspect near the middle of the alveolar bone.
4. The observations from this study highlight the importance of assessing the mandibular premolars during orthodontic treatment in Class I subjects of different vertical facial types.
 XML Download
XML Download