

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Gummy smile appears most frequently among women aged 20-30 years.1 With an increasing number of adult female orthodontic patients,2,3 corrective treatment for a gummy smile has become important in the field of orthodontics. The goals of orthodontic treatment are not limited to simply achieving even teeth and well-occluded maxillo-mandibular dental arches. Such treatment also aims to provide a beautiful smile line that harmonizes with the face.4,5 In recent years, the increasing emphasis on a beautiful smile has increased the interest in treating a gummy smile using anterior-teeth intrusion.
Most patients with a gummy smile show excessive vertical growth of the maxillary bone.6,7 Patients with vertically overdeveloped maxillae have not always had good results from treatment by tooth extraction; frequently, gum exposure is actually increased after such attempts at correction. In contrast, anterior tooth intrusion using a miniscrew implant can provide good results because the surgeon can control the degree of gum exposure.8,9,10,11,12,13,14
Many studies have assessed cortical bone thickness in the molar and premolar areas and in the midpalatal area for placement of miniscrew implants.15,16,17,18,19,20 In addition, recent clinical research findings on treatment with miniscrew implants at the maxillary anterior alveolar bone have been reported8,9,10,11,12,13,14 However, there is limited basic anatomical research aimed at determining the optimal placement of miniscrew implants.
This study aimed to evaluate the quality of maxillary anterior alveolar bone toward the goal of optimal miniscrew implant placement. Clinical guidelines were developed by measuring cortical-bone and labio-palatal thickness and interdental root distance using cone-beam computed tomography (CBCT).
MATERIALS AND METHODS
Subjects
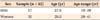
Diagnostic CBCT (Point 3D Cmobi 500C; Pointnix, Seoul, Korea) was conducted for patients who visited the private dental clinic (Seoul, Korea) to receive orthodontic treatment. Inclusion criteria for this study were as follows: no maxillary anterior cross-bite observed in clinical or radiographic tests; maxillary anterior crowding less than 2-3 mm; no maxillary anterior loss or microdontia; maxillary anterior spacing within 2 mm; completion of growth without orthodontic treatment; and no moderate or severe periodontitis. We included 52 subjects with an average age of 27.9 years. The study cohort included patients with skeletal Cl I, Cl II, and Cl III and comprised 17 men (mean age, 27.6 years) and 35 women (mean age, 28.0 years) (Table 1). All patients provided informed consent for the use of their CT data in this study, which was approved by the KONIBP (Korea National Institute for Bioethics Policy, P01-201306-RS-01-00).
Measurements
The CBCT examinations were carried out after a vertical beam was fit to the central line of the patients' faces in the natural head position (NHP), in which they look at a mirror placed in front of the machine (Figure 1). The Digital Imaging and Communications in Medicine (DICOM) files obtained through CBCT (voxel size, 0.160 mm; field of view, 12 × 9 cm) were analyzed using OnDemand3D (Cybermed Inc., Seoul, Korea), a 3-dimensional (3D) analysis program. The reference planes for 3D analysis were the vertical and horizontal planes of the NHP obtained using CBCT. The horizontal plane was used as the reference plane for measurements (Figure 2).
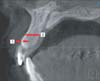
Three interdental root regions were measured: between the maxillary central incisors (U1-U1), between the maxillary central incisor and the lateral incisor (U1-U2), and between the upper central incisor and the canine (U2-U3). For the regions U1-U2 and U2-U3, the site to the left or right with the least crowding was measured. In parallel with the reference line, the cortical bone thickness on the labial side, the labio-palatal thickness, and the interdental root distance were measured at the 4 mm, 6 mm, and 8 mm levels apical to the interdental cementoenamel junction (ICEJ) (Figures 3,4,5).
Statistical analysis
Measurement and analysis of the data were carried out by a single researcher. To assess intra-examiner reliability, specimens were randomly extracted, and measurements were repeated 2 times at an interval of 1 week. No statistical differences were observed between the two sets of measurements (p > 0.05).
The data were analyzed using the SAS 9.2 Statistical Package program (SAS Institute, Cary, NC, USA). Because the data showed non-normal distribution, median and interquartile ranges (IQR) were used instead of mean and standard deviation, and the Kruskal-Wallis Test was used to evaluate differences between and within the 3 regions.
RESULTS
Cortical bone thickness
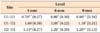
Cortical bone was significantly thicker in the U2-U3 region than in the U1-U1 region. For all measured regions (U1-U1, U1-U2, and U2-U3), the cortical bone thickness tended to get thicker moving apically toward the ICEJ, and there was a significant difference between the 4 mm and 8 mm levels in the U1-U1 and U2-U3 regions (p < 0.05). In particular, the U1-U1 region showed significantly thinner cortical bone, measuring about 0.70-0.80 mm (p < 0.05) (Table 2, Figure 6).
Labio-palatal thickness
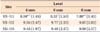
The labio-palatal thickness was greatest in the U1-U2 region and was significantly less in the U1-U1 region (p < 0.05). In the U1-U1 region, the labio-palatal thickness decreased apically to the ICEJ; in particular, there was a significant difference between the 4 mm and 8 mm levels apical to the ICEJ (p < 0.05) (Table 3, Figure 7).
DISCUSSION
In the past, orthodontic treatment for gummy smile or deep overbite was considered very difficult. In severe cases, orthognathic surgery was usually recommended, and the more conservative choice of orthodontic treatment alone did not always yield good aesthetic results, namely, gum exposure is frequently increased after such attempts at correction.14
For cases involving premolar extraction, the application of additional intrusion force after placing a miniscrew implant into the maxillary anterior region yields good results in patients with a gummy smile and a long face.8,9,10,11,12,13,14 In non-extraction patients with a deep bite, satisfactory results can be obtained by applying intrusion force toward the center of resistance after placing a miniscrew implant between the lateral incisor and the canine.8,9,10,11,12,13,14 Thus, the use of miniscrew implants in the maxillary anterior region is essential for treating gummy smile or anterior deep overbite.
Two clinical approaches that affect the stability of the current miniscrew implant are presently used.18 The first approach is to wait for osseointegration after placing a miniscrew implant and subsequently applying orthodontic force. In this approach, the quality of spongy bone is more important than cortical bone thickness.21,22 However, osseointegration takes time, so orthodontic force cannot be applied immediately. The second approach is to apply orthodontic force immediately after placing a miniscrew implant, before osseointegration occurs. In this approach, cortical bone thickness plays a more important role than bone quality in obtaining sufficient mechanical interaction between the miniscrew implants and bone. Many studies suggest that cortical bone thickness is the most important determinant of initial stability.23,24,25,26,27,28,29,30,31,32,33,34 For orthodontic correction, the initial stability provided by cortical bone thickness is a very important factor because the force is added just after implantation or within 1 to 3 weeks thereafter.
We observed that the cortical bone thickness at levels 4 to 8 mm apical to the ICEJ were 0.70 ± 0.27 to 0.90 ± 0.30 mm in the U1-U1 region, 1.00 ± 0.32 to 1.10 ± 0.21 mm in the U1-U2 region, and 1.15 ± 0.27 to 1.20 ± 0.13 mm in the U2-U3 region. According to Farnsworth et al.20, the cortical bone thickness was 1.33 ± 0.24 mm in the U4-U5 region, 1.45 ± 0.28 mm in the U5-U6 region, and 1.26 ± 0.24 mm in the U6-U7 region. We observed that the cortical region of the maxillary anterior alveolar bone was thinner than that of the buccal premolar and molar regions. In particular, the region between the maxillary central incisors (U1-U1) showed a cortical bone thickness as small as 0.70-0.90 mm. Nevertheless, in practice, miniscrews are implanted in this region without any big problems in stability.8,9,10,11,12,13,14 An orthodontic force about 200-250 g is applied for retraction of anterior teeth, while a force of only 50-100 g is necessary for anterior tooth intrusion; thus, this relatively weak force does not cause stability problems.35,36
In addition to cortical bone thickness, other factors affecting the stability of miniscrew implants should be considered. Davies37 described the process of post-implant bone healing by contact osteogenesis and distant osteogenesis in spongy bone. Contact osteogenesis is the process whereby osteoprogenic cells originating from blood (medulla) attach to the surface of the miniscrew implant, forming a group. These cells change into osteoblast cells to form bone in the direction of the existing bone on the surface of the implant. Because this new bone is formed immediately at the surface of an implant, it plays a very important role in the initial and early stability of the implant.37 Distant osteogenesis takes place in existing bone, with growth toward the surface of the miniscrew. If contact osteogenesis is not satisfactory early in the healing process, stabilization of the bone will take longer because the bone must be formed entirely by distant osteogenesis; poor initial stability can thus cause implant failure. Davies37 suggested that the success of implants in thin or poor cortical bones (Cl III and Cl IV bones) depends on adequate contact osteogenesis.
Moon et al.38 and Kuroda et al.39 reported that while mandibular cortical bone is thicker than maxillary posterior alveolar bone, the success rate of implantation into the latter is similar to or higher than that of the mandibular molar region. Because factors related to spongy bone blood supply are reduced in the mandible as compared to the maxilla, the latter is a more favorable environment for contact osteogenesis in spongy bone. Thus, contact osteogenesis is an important factor determining miniscrew implant stability.
The labio-palatal thickness was greatest in the U1-U2 region and least in the U1-U1 region. In the U1-U1 region, the labio-palatal thickness decreased apically toward the ICEJ. In particular, there was a significant difference between the 4 mm and 8 mm levels. This trend relates to the incisive foramen, starting at the height of about 6 mm. Thus, the safe placement length for miniscrew implants placed in the U1-U1 region is thought to be 7-8 mm. In addition, at the 6 mm and 8 mm levels, the displacement of measurement values in the U1-U2 and U2-U3 regions appears to be relatively larger than that in the U1-U1 region. This observation indicates that the difference in displacement of labio-palatal thickness in the U1-U2 and U2-U3 regions was severe, as the difference depends on the depth of the maxillary palatal vault. Thus, if the palatal vault is deep, miniscrews with a length about 6-7 mm would be best for fixing miniscrew implants in the U1-U2 and U2-U3 regions.
The interdental root distance at the 4 mm and 8 mm levels was 2.37 ± 0.67 to 3.87 ± 0.99 mm in the U1-U1 region, 1.90 ± 0.41 to 2.95 ± 0.90 mm in the U1-U2 region, and 2.80 ± 0.68 to 3.88 ± 0.84 mm in the U2-U3 region. Regarding the mesiodistal dimension, Schnelle et al.15 suggested that at least 3 mm of interradicular space would be required for safe placement of a miniscrew implant. Poggio et al.40 also emphasized maintaining enough interradicular space to protect periodontal health and ensure implant stability. A minimum clearance of 1 mm of bone around the miniscrew implant has been recommended for safety.24 However, Janson et al.41 recently proposed that the proximity of roots to miniscrew implants did not influence the stability or success rate when the distance between the miniscrew implant and dental root indicated no periodontal ligament invasion. Wider interradicular space can be achieved because miniscrew implants are generally placed at angle of about 60°-80°, but not perpendicular to cortical bone. The diameter of commonly used miniscrew implants is 1.2-1.6 mm. Considering the interdental root distance, this diameter poses no problem for maxillary anterior implants; however, especially for placement in the U1-U2 region, miniscrew implants with a diameter of 1.2 mm or 1.0 mm will be safer.
CONCLUSION
The region between the maxillary lateral incisor and the canine (U2-U3) should be the first choice for miniscrew implantation into maxillary anterior interdental alveolar bone. This choice is optimal regarding cortical bone thickness, interdental root distance, and labio-palatal thickness. However, this region requires the placement of 2 miniscrew implants in total, one on the left side and one on the right side. Alternatively, the region between the maxillary central incisors (U1-U1) may be considered the second best site, as intrusion of the maxillary anterior teeth is possible just with one miniscrew implant.







 XML Download
XML Download