

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Expanded medical coverage and governmental policies for low medical costs have decreased the economic burden of hospital-based care in Korea.1 In addition, improved standard of living and heightened interest in health and medical issues have increased the demand for healthcare,2 while advanced information and communication technologies have enabled the public to obtain more medical information. These changes have led to increased medical disputes.3 For example, 85 medical accident cases were litigated in 1990, whereas 882 cases (an almost 10-fold increase) were legally contested in 2002.4
This trend is also observable in dentistry.5 According to the Korean Consumer Protection Board,6 dental disputes constituted 926 and 2,388 of the counsels in 1996 and 2004, respectively; in the first half of 2005, such disputes accounted for most of the medical litigations. Further, compensation for damages is rising by 25.1% annually.1 The increasing number of dental disputes heightens the need to analyze the underlying factors in the orthodontic field.
A committee of the Korean Association of Orthodontists developed and applied a questionnaire to identify factors related to medical accidents among members in 1998.2 A similar investigation was repeated in 2011. Here, we report the results of the 2011 survey of medical accident-related factors in orthodontics.
MATERIALS AND METHODS
The questionnaire consisted of three categories with 56 items to obtain the relevant information. The healthcare provider-related information included gender, age, geographic area of practice, type of facility, duration of practice, orthodontic training, total number of orthodontic patients, weekly sessions of orthodontic practice, and number of orthodontic patients per session. The patient-related information included patient age, chief complaint, diagnosis, severity of malocclusion, duration of treatment, subject of the dispute, and occupation, age, and standard of living of the complainant.
The questionnaire also covered the cause of the medical accident from the provider's and complainant's viewpoints, time of occurrence of the accident (based on the clinic opening time), existence and cause of medical negligence, experience of lock-in, resolver of the dispute, amount of indemnity, and time until settlement. Furthermore, it addressed whether advice was sought, the result of such inquiry, and the provider's psychological state after the dispute.
The items related to precautions during orthodontic treatment and medical record maintenance were methods for evaluating systemic diseases, types of diagnostic data, use of computers in diagnosis, frequency of explanation before treatment, and time taken for diagnosis. The frequency of agreement before treatment, methods used to explain treatment fees, frequency of documenting and retaining medical records, frequency of taking radiographs, and method for managing patients with prolonged clinical absence were also recorded. Finally, opinions about increasing dental disputes and the necessity of continuing education and creating a system for dealing with conflicts were sought. Availability of coverage for compensation and satisfaction with the amount were also noted.
The questionnaire was distributed to 1,600 members of the Korean Academy of Orthodontics by mail, with a return envelope enclosed. For several questions, the respondents were allowed more than one answer. The analysis excluded questions with missing answers or multiple responses where a single answer was required. Associations between experience of medical accidents and the other recorded data were statistically analyzed by the chi-square test. p < 0.05 indicated a significant difference. For statistical analysis, the SPSS 15.0 program (SPSS Inc., Chicago, IL, USA) was used.
RESULTS
Healthcare provider-related findings
In August 2011, 369 members (237 men and 130 women) of the Korean Association of Orthodontists completed the questionnaire. Of these respondents, 101 (27.5%) had experienced medical accidents (experienced group), whereas 266 (72.5%) had not (inexperienced group).
Gender
The experienced group included 70.3% male and 29.7% female respondents, and the inexperienced group comprised 62.4% male and 37.59% female respondents. The chi-square test did not show significantly different experience of medical accidents between the genders (p = 0.1581).
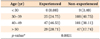
Age
In the experienced group, 24.7% were in the 30-40 age group, 46.5% were aged between 40 and 50 years, and 28.7% were over 50 years old. Among the 30-40 year olds, 16% fewer respondents had experienced medical accidents than those who had not. In contrast, among the respondents aged 40-50 years, 8.4% more had experienced medical accidents than those who had not. Experience of medical accidents significantly differed among the age groups (Table 1).
Geographic area of practice
In the experienced group, 64% of the respondents practiced in Seoul and Gyeonggi. A high rate of medical accidents was also reported in big cities such as Busan, Daejeon, Daegu, and Incheon. However, experience of medical accidents did not significantly differ among the areas (Table 2).
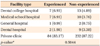
Type of facility
Among the experienced respondents, 83.2% worked at private clinics, whereas 1.0-6.9% worked at dental college hospitals, medical school hospitals, dental hospitals, and general hospitals. Experience of medical accidents did not significantly differ according to the facility type (Table 3).
Duration of practice
Two-thirds (63.6%) of the experienced respondents had been in clinical practice for over 10 years and 23.3% had been practicing for 5-10 years. Experience of medical accidents significantly differed according to the duration of practice (Table 4).
Orthodontic training and number of patients
With regard to orthodontic training, 77% and 23% of the respondents in the experienced group were and were not trained in orthodontics, respectively. In the inexperienced group, 64.9% had received orthodontic training but 35.1% had not. Experience of medical accidents significantly differed between the trained and the untrained respondents (p = 0.0269; Table 5).
Patient-related findings
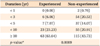
Chief complaint, diagnosis, and severity of malocclusion
The chief complaints of 32.3% and 25.4% of the patients were crowding and protrusion, respectively. The healthcare providers diagnosed 50%, 26%, and 24% cases of Class I, II, and III malocclusion, respectively. The most common diagnosis was Class I crowding (33%). Malocclusion was considered severe in 29.1% of the cases, moderate in 58.7%, and mild in 12.2%.
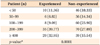
Age, complainant data, and subject of the dispute
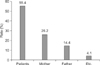
Of the patients who experienced medical accidents, 47.3% were over 25 years old, whereas the others were aged 19-24, 13-18, or under 12 years (Figure 1). The complainant was the patient in 55.4% of the cases and the patient's parents in 40.6% of the cases (Figure 2). The subject of the dispute was mainly dissatisfaction with appearance (18.6%), followed by root resorption, pulpal necrosis, temporomandibular disorder, inappropriate occlusion, and accidents during extraction (6.8-9.7%) (Figure 3).
Dispute-related findings
Resolution of the dispute
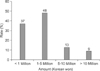
In most cases (85%), the dispute was settled by the healthcare provider alone for less than 5 million Korean won (KRW). Compensation over 10 million KRW was uncommon (9%) (Figure 6). The time until settlement was 1.3 years in 41.5% of the cases (Figure 7). The respondents sought advice from colleagues (44%), elders (18%), and professors (11%) (Figure 8). Most felt that these inquiries were helpful, but 20% of the respondents found that the advice was not helpful or even exacerbated the problem.
Preventive measures in orthodontic treatment
Medical record maintenance
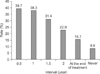
Data for orthodontic diagnosis were obtained from lateral cephalograms, panoramic radiographs, dental models, and clinical photographs. Of the respondents, 74.2% used a computer for diagnosis and 65% used documents that were explained by other clinicians or assistants. During orthodontic treatment, 78% of the respondents took radiographs every 6-12 months, 15.7% took radiographs at the end of treatment, and 0.9% did not take radiographs at all (Figure 9).
Precautions during orthodontic treatment
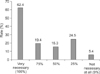
Of the respondents, 62.4% expressed a strong need for continuing education regarding medical accidents or disputes, and 76.3% felt that a system for settling such disputes is greatly required (Figures 10 and 11). Further, 55.8% had coverage for compensation, but only 23.5% were satisfied with the amount of coverage (Figure 12).
DISCUSSION
The percentage of respondents who experienced one or more medical accidents (27.5%) in the 2011 survey is similar to that in the 1998 survey.2 However, it is lower than the percentage of general dentists who experienced medical accidents (47.9%) in another survey.4 In the experienced group, 81% had one or two medical accidents and only 2% had more than six accidents.
When compared with the 1998 results, an increased number of women experienced medical accidents in the 2011 survey.2 In a previous study,2 49.8% of the male respondents and 39% of the female respondents experienced medical accidents. Further, the respondents who experienced medical accidents tended to be older in the 2011 survey (40-50 years old) than in the 1998 survey (30-40 years old).
In the 2011 survey, 63.6% of the respondents who experienced medical accidents had been practicing for over 10 years, indicating that greater skill and proficiency through prolonged practice may not prevent medical accidents. In contrast, 78.3% of the medical accidents occurred within the first 5 years of practice and the rate decreased with a longer duration of practice in the 1998 survey.
The majority (64%) of the 2011 respondents who experienced medical accidents practiced in Seoul and Gyeonggi. The lack of a significant difference in the experience rate among the areas may be explained by the inadequate number of respondents in certain regions for statistical analysis. Regarding the type of facility, 83.2% of the 2011 experienced respondents worked at a private clinic. Comparison with the 1998 results showed that the number of medical accidents in dental hospitals increased along with increase in the number of dental hospitals. The incidence of medical accidents did not significantly differ among the hospital types, possibly because the number of facilities other than private clinics was too small to show a significant difference.
The rate of orthodontically trained respondents with experience of medical accidents was higher in the 2011 survey (77%) than in the 1998 survey (61%). Further, a significantly higher incidence of medical accidents was noted among the orthodontically trained 2011 respondents than those without such training. The previous study of general dentists showed no significant difference in experience of medical accidents between the trained and the untrained groups. Therefore, the tendency observed in the present study may be characteristic of orthodontic clinics.
The respondents judged the malocclusion to be moderate or mild in most of the cases, showing that medical accidents occur not only in difficult cases but also in simple routine cases.
Of the patients involved in medical accidents, 47.3% were over 25 years old, which may explain why more disputes were raised by the patients themselves in the later survey than in the 1998 survey (mainly 13-18 years old). The most common basis of medical accident claims in the 2011 study was dissatisfaction with appearance (18.6%), whereas root resorption was the main cause of such claims in the 1998 survey.
According to the 2011 respondents, the patients thought that the main cause of the dispute was negligence of medical staff, but they considered the dispute to be caused by the patient's lack of understanding. These results suggest insufficient communication between healthcare providers and patients.7 Only 27.2% of the healthcare providers admitted medical negligence, showing a strong decrease from the 1998 survey (46%). This finding may suggest that patients now more frequently raise disputes in instances without medical negligence. In a previous study, 21.4% of the dental disputes were insufficiently explained, which was a higher percentage than that in other medical departments.3,8 Clinical demonstrations occurred in 14.1% of the 2011 disputes, showing an over two-fold increase from the 1998 survey and suggesting a rise in violent reactions to medical accidents in orthodontic practice.
Previous studies showed that the average compensation was 93,260,000 KRW for settlement of lawsuits in all medical fields and 10-30 million KRW for dental disputes.8-10 Contrarily, the 2011 results showed that dental disputes in the orthodontic field are settled for a relatively low amount (less than 5 million KRW).
No respondents sought advice from lawyers in the 1998 survey; however, 9% of the 2011 respondents did. This change indicates increasing pursuit of legal settlement by healthcare providers and coincides with the rising tendency toward litigation for dental procedures. According to Shin,3 eight lawsuits were filed between 1994 and 1999, whereas 22 were filed from 2000 to 2004.
Most of the 2011 respondents considered that they explained their diagnosis well to the patients, and 49% reported that they spend more than 25 minutes on a diagnosis. Most also thought that explanation and agreement of a diagnosis are important in the event of a dispute. Of the 2011 respondents, 65% used documents explained by other doctors or assistants (Figure 13), whereas only 15% of the 1998 respondents used such documents. This difference is likely attributable to the general opinion that healthcare providers should carefully explain the treatments and maintain appropriate records to prevent disputes.11,12
Of the 2011 respondents, 62.4% felt an extreme need for continuing education regarding dental disputes and 76.3% felt that a system for settling dental disputes is necessary. These findings are similar to the results of the 1998 survey, indicating a lack of improvement in continuing education or dispute-processing systems despite other improvements in the dental care environment.13 More than half of the respondents had coverage for compensation responsibility, but less than 25% were satisfied with the amount of coverage. The reasons for this discontentment included inadequate managing capability, insufficient methods of reception and management, and deficient expense compensation.
CONCLUSION
The 2011 survey showed some similar findings to the 1998 survey. Therefore, the need for continuing education on dental disputes and systems for settling such disputes has not yet been met. Advances in education and countermeasures for preventing and managing medical accidents and disputes in orthodontic practice are necessary.14 Future studies should focus on how to meet these needs in the field of orthodontics.










 XML Download
XML Download