

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The placement of fixed orthodontic appliances increases the difficulty in mechanical plaque removal and thus predisposes orthodontic patients to plaque accumulation and enamel demineralization.1-3 Fixed orthodontic treatment is also associated with increased probing pocket depths, elevated bacterial count in plaque, and a shift in the healthy microbial composition of subgingival plaque to a periodontal pathogenic one.4-6 Therefore, optimal oral home care and professional prophylactic programs are of paramount importance in patients undergoing fixed orthodontic treatment.7,8
During professional oral hygiene procedures, ultrasonic scalers are used around the bracket base, a critical site of plaque accumulation, and can affect the bracket-enamel interface.9,10 Prolonged ultrasonic vibration at maximum power is used to facilitate the removal of posts, crowns, or bridges and could similarly debond orthodontic brackets.11-15 This action is attributable to the propagation of vibrations from the ultrasonic device to the object that is to be removed, as well as to the biophysical action of ultrasound within the coolant (i.e., cavitational activity and acoustic microstreaming).16 However, to date, no study of the effects of ultrasonic instrumentation for oral hygiene maintenance on the shear bond strength (SBS) of orthodontic brackets has been conducted.
The aim of this study was to evaluate the effects of ultrasonic instrumentation with different scaler-tip angulations on the SBS and bond failure mode of metallic orthodontic brackets.
MATERIALS AND METHODS
Specimens
Seventy-two premolars extracted for orthodontic reasons from patients aged 12 - 18 years were collected after receiving adequate informed consent. The teeth did not have cracks visible under ×4 magnification, hypoplasia, white spots, caries, or labial restorations.17 They were washed in water to remove contamination and stored in distilled water in a refrigerator (i.e., nominal 4℃) for 1 - 6 months, in accordance with the ISO/TS 11405 standard.18
Bonding procedure
In strict accordance with the protocol described by Alessandri Bonetti et al.,19 the labial enamel surfaces were cleaned, polished, and etched. A thin uniform coat of primer (Transbond XT; 3M Unitek, Monrovia, CA, USA) was applied by using a microbrush. Adhesive pre-coated metallic brackets (APC II adhesive coating on Victory Series brackets; 3M Unitek) were then placed on the teeth, adjusted to their final positions, and pressed firmly. After removing excess resin from the periphery of the bracket base with a dental probe, the adhesive was cured by using a light-emitting diode light source (Ortholux luminous curing light; 3M Unitek) for 6 s (3 s mesially and 3 s distally), according to the manufacturer's instruction.
Mounting procedure
After storage in distilled water at 37℃ for 24 h (ISO/TS 1140518; test type 1: short-term test), the teeth were embedded in autopolymerizing acrylic resin (Orthocryl; Dentaurum, Bologna, Italy) in polyvinyl chloride molds (15-mm diameter and 20-mm height) so that the roots were fully embedded in acrylic resin and the bonding surface of the brackets remained perpendicular to the horizontal plane and parallel to the direction of the force to be applied, in an effort to minimize peel and maximize shear during testing. To ensure the fulfillment of these requirements, the roots of each tooth were initially inserted in a wax pedestal, which was molded until the correct position was achieved and verified with the aid of a parallelometer (Paraline; Dentaurum).
Ultrasonic instrumentation
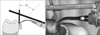
The teeth were randomly divided into 3 groups of 24 specimens each: control group, no treatment; 45°-angulation group, ultrasonic instrumentation with a scaler-tip angulation of 45° (Figure 1); 0°-angulation group, ultrasonic instrumentation with a scaler-tip angulation of 0° (Figure 2).
To maintain the desired angulation in the 45°-angulation group, an external support with a component forming an angle of 45° to the scaler tip was fastened to the ultrasonic device and the component was maintained parallel to the tooth surface, thus achieving an angle of 45° between the scaler tip and the tooth surface.
A piezoelectric ultrasonic scaler (Piezosteril 5; Castellini, Bologna, Italy) was used with insert "C1" (recommended by the manufacturer for supragingival scaling) at a power setting of 7.5 W. Tap water, delivered directly from the dental unit, was used as the coolant. Ultrasonic instrumentation was performed for 1 min, with 20 s each on the mesial, distal, and occlusal sides of the bracket base. The gingival side of the bracket base was omitted because the roots were embedded in acrylic resin up to the cementoenamel junction, preventing the access of the scaler tip to that surface. The bracket slot was not instrumented because the bracket wings did not allow the chosen scaler-tip angulations to be consistently achieved along that surface. A single experienced and trained operator performed all these procedures.
Debonding procedure
After storage in distilled water at room temperature for 24 h, the specimens were tested according to the ISO/TS 1140518 standard in a universal testing machine (Instron, Milan, Italy). Each acrylic block was placed in the machine so that the bracket base was parallel to the direction of the force to be applied and a chisel-shaped blade was placed on the occlusal side of the ligature groove between the bracket base and the wings. A shear debonding force was applied in the occlusogingival direction at a crosshead speed of 1 mm/min,18 and the amount of shear force required to debond each bracket was recorded in newtons. Stress values were calculated as the ratio of the debonding load (in newtons) to the area of the bracket base (9.79 mm2) and measured in megapascals (MPa).20
Failure analysis
To evaluate the mode of bond failure, the specimens were examined at ×20 magnification with an optical microscope.21 By using open-source image-analysis software (ImageJ; National Institutes of Health, Bethesda, MD, USA), the amount of adhesive remaining on the tooth was expressed as a percentage of the total bonded area.19 The analysis was performed by an examiner trained to use the software and blinded to the groups. The evaluations were repeated by the same examiner 1 week later; if any discrepancies arose, a third assessment was performed to determine the final score.
An adhesive remnant index (ARI) score was assigned to each specimen: 0, no adhesive left on the tooth; 1, less than half of the adhesive remained on the tooth; 2, more than half of the adhesive remained on the tooth; 3, all the adhesive was left on the tooth, with a distinct impression of the bracket mesh.22,23
Statistical analysis
Statistical analyses were performed by using statistical software (PASW Statistics for Windows, version 18.0; IBM Co., Armonk, NY, USA). The significance level was set at 0.05.
A pilot study estimated the expected difference in the mean SBS values between the untreated and the treated specimens as 2.3 MPa and the within-group standard deviation as 2.4 MPa. Given the α level of 0.0167 (Bonferroni adjustment for multiple comparisons) with a power of 80%, a minimum number of 24 specimens was required for each group.
The Shapiro-Wilk test showed that the SBS data were consistent with a Gaussian distribution in the control and 0°-angulation groups, but they were not normally distributed in the 45°-angulation group. Therefore, Kruskal-Wallis test was used to evaluate these data. Pairwise comparisons were performed by using the Mann-Whitney U-test with Bonferroni correction (adjusted α level = 0.0167). The Kruskal-Wallis test was also used to assess the significance of the differences in the ARI scores among the groups.
RESULTS
The results of the debonding test are shown in Table 1. Three specimens of the 0°-angulation group could not be tested because debonding of the brackets occurred during ultrasonic instrumentation. In these cases, an SBS value of 0 MPa was attributed because it was considered more representative of the clinical situation than a value obtained by interpolation or considering the loss of the specimen.
A significant difference in the mean SBS values was noted among the groups (p = 0.004). The mean SBS value of the control group (9.92 MPa) was significantly higher than that of the 45°-angulation (7.77 MPa; p = 0.004) and 0°-angulation (7.16 MPa; p = 0.006) groups. However, the mean SBS values of the treated groups were not significantly different.
The distribution of the ARI scores is shown in Figure 3. The Kruskal-Wallis test showed no significant differences among the groups. In many specimens (62.5% of the 45°-angulation group and 66.67% of the control and 0°-angulation groups), most of the adhesive remained on the enamel (ARI scores of 2 or 3).
DISCUSSION
Proper professional oral hygiene maintenance is of paramount importance in patients undergoing fixed orthodontic treatment to reduce the risk of periodontal diseases and enamel demineralization.1-3 Ultrasonic instrumentation is usually carried out around the bracket base, which is a critical site of plaque accumulation,9,10 but no studies have been performed yet to assess whether there is any influence on the SBS and mode of bond failure of metallic orthodontic brackets.
To simulate extreme conditions and highlight the most detrimental effect of ultrasonic instrumentation on the SBS of metallic orthodontic brackets, the time of instrumentation was overrated when compared with a routine clinical procedure, in which the scaler tip probably contacts the bracket-enamel interface for only a short period. Therefore, 1 minute was chosen as the total application time.24 Further, because manufacturers generally recommend a power setting of medium to high for supragingival scaling and Chapple et al.25 demonstrated that a half power setting is as effective as a full one, a power setting of 7.5 W (50% of the maximum power [15 W] of the device) was selected in this study. Finally, the experienced operator who performed all the ultrasonic procedures had been trained to maintain the force of scaler-tip application as low as possible while contacting the bracket in a consistent manner, similarly to the routine clinical setting. However, as this method is not a standardized way of force application, it may limit the reproducibility of the study. In this study, ultrasonic instrumentation around the bracket base decreased the SBS of the metallic orthodontic brackets compared with the control specimens. The mean SBS values of both the treated groups were still beyond 6 MPa, which is reportedly adequate for orthodontic purposes.26 However, such a reduction is undesirable because it increases the risk of bracket failure after professional oral hygiene procedures, consequently impeding treatment progress and prolonging treatment time.27
The angulation of the scaler tip has been investigated in relation to the potential damage to the tooth surface but not to the impairment of the SBS of metallic orthodontic brackets. The extent of damage to the tooth surface is reportedly the highest with a tip angulation of 45° when using piezoelectric ultrasonic scalers.28,29 In this study, no significant differences in the SBS were found between the 0°-angulation and the 45°-angulation groups, suggesting that the tested angulations did not influence to bracket bond failure after professional oral hygiene procedures. However, the scaler tip should preferably be parallel to the tooth surface (i.e., 0° angulation), or at an angle less than 15°, to orient the pattern of ultrasonic vibration parallel to the tooth surface and decrease the risk of damage.28,29 Interestingly, 3 brackets detached in the 0°-angulation group before the SBS testing; the reason for their failure is not fully understood.
Finally, the ARI scores were similar among the groups, indicating that ultrasonic instrumentation did not affect the mode of bracket bond failure. In all the groups, most of the adhesive remained on the enamel, indicating a low risk of enamel damage after debonding.
Further studies are required to evaluate the influence of other parameters (e.g., power setting, load, instrumentation time) pertaining to ultrasonic instrumentation for oral hygienic purposes on the SBS of orthodontic brackets.
CONCLUSION
Under the conditions of this in vitro study, 1 minute ultrasonic instrumentation around the bracket base at medium power reduced the SBS of metallic orthodontic brackets, indicating a higher risk of bracket bond failure after professional oral hygiene procedures. Therefore, clinicians should avoid prolonged ultrasonic instrumentation around the bracket base during plaque removal. The scaler-tip angulation does not influence the SBS reduction and failure mode of metallic orthodontic brackets.



 XML Download
XML Download