

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Physical attractiveness is an important social issue in our culture, and the face is one of its key features.1 Facial attractiveness and smile attractiveness appear to be strongly connected to each other, since attention is mainly directed toward the mouth and eyes of the speaker's face in social interactions. The mouth is the center of facial communication, and the smile plays important roles in facial expression and appearance.2 The demand for improved dental appearance is one of the major motives of orthodontic treatment. Many adults and adolescents perceive their smile as unpleasant and seek orthodontic treatment in order to improve it. An esthetically pleasing smile is not only dependent on components such as tooth position, size, shape, and color, but also on the amount of gingiva displayed and the framing of the lips.3 All these components form a harmonic and symmetric entity.
Kokich and colleagues4 were the first to use computer-based image alterations to quantify the acceptability of smile characteristics. Because of the consistency of variable manipulation and controlled presentation, computerized alteration appears to be an effective method to explore esthetics. Through this method, it was possible to assess the perceptive abilities of dentists and laypersons under various conditions such as dental midline shift, asymmetry of crown width/height, canting of the occlusal plane, buccal corridor minimization, and excessive gingival display, and showed that these factors affected the attractiveness of the smile.4,5,6 Among these factors, laypersons showed different perceptive abilities in maxillary to mandibular midline discrepancy, asymmetrical central incisor crown length, lateral incisor width, and canting of the occlusal plane compared to dentists, demonstrating a larger acceptable range.
Esthetic perception varies from person to person and is influenced by each person's experiences and social environment. Miller7 stated that the trained and observant eye readily detects that which is out of balance and not in harmony with its environment. There are several studies reporting that not only level of education, but also gender, age, and culture can influence the esthetic perception of dental features.8,9,10,11,12,13 However, there are few studies regarding the effects of orthodontic treatment experience on esthetic self-perception. Tuominen et al.14 reported that after orthodontic treatment, adult patients showed higher perception in treatment demand than others who did not receive orthodontic treatment. Kerosuo et al.15 and Bernabé et al.16 reported that orthodontic treatment had a positive effect on the self-perception of dental treatment needs in young adults. The studies used the aesthetic component of the Index of Orthodontic Treatment Need and visual analog scale (VAS), respectively, and reported that treated young adults showed a higher self-perception of dental appearance. Feu et al.17 found that in adolescents, orthodontic treatment with a fixed appliance significantly improved esthetic self-perception. However, these studies focused largely on evaluating gross esthetic discrepancies related to debilitating malocclusions by using various intraoral photographs of anterior dental crowding, crossbite, and so on. Moreover, a previous study18 examined the perception of esthetic smile components such as gingival exposure and maxillary dental midline deviation by laypersons with and without orthodontic treatment by using only 3 modified images for the evaluation of these variables.
The purpose of this study was to examine whether the experience of orthodontic treatment affects the individual's perception of smile esthetics and to evaluate differences among orthodontically treated patients, non-treated laypersons, and dentists by using computerized image alterations.
MATERIALS AND METHODS
Three groups were included in this study. The non-treated layperson group (group 1: n = 50, 12 men and 38 women; mean age, 22.0 ± 2.9 years) consisted of Wonkwang University (Iksan, Korea) college students who had never received orthodontic treatment. The treated layperson group (group 2: n = 50, 6 men and 44 women; mean age, 23.8 ± 3.6 years) consisted of patients who had completed orthodontic treatment at Wonkwang University Dental Hospital (Iksan, Korea). The dentist group (group 3: n = 30, 17 men and 13 women; 27.4 ± 5.1 years) consisted of residents at Wonkwang University Dental Hospital.
A photograph of a posed smile of young Korean woman was digitally altered by using Adobe Photoshop (version CS3; Adobe Systems, Inc., San Jose, CA, USA). Variables such as maxillary right central incisor gingival margin height, maxillary left lateral incisor crown width and length, incisal plane canting, and dental midline shift were altered gradually from the original photograph. After manipulation, the nose and chin were erased to reduce the number of variables in the images. However, for the dental midline shift, part of the nose was left to help evaluate the facial midline.
Four gradual alterations were produced from the original photograph for each variable. The clinical crown length of the maxillary right central incisor was shortened in 0.5-mm increments by changing the free gingival margin while maintaining the incisal edge at the same level (Figure 1). The maxillary left lateral incisor crown width and length were altered in 1.0-mm increments. As the crown width decreased, the gingival margin moved incisally while the crown width/height proportion was maintained (Figure 2). Canting of the incisal plane was manipulated by altering the plane from the right canine to the left canine (Figure 3). Since it was impossible to see the interpupillary line in the photographs, the lower lip line and incisal plane were positioned parallel to the lower border of the original photograph as a reference. By rotating around the central point of the incisal embrasure between the central incisor crowns, gradual canting was performed in 1.0-mm increments for the entire anterior dental segment while positioning the left side inferior and the right side superior. The maxillary dental midline was shifted to the patient's right side in 0.5-mm increments, and the mandibular dental midline was shifted to the patient's left side in 0.5-mm increments, for a total of 1.0 mm of gradual change while keeping the adjacent soft tissue intact (Figure 4).
The 20 photographs, consisting of 16 digitally altered photographs and 4 original images, were compiled into a catalog of 5 pages. Each page comprised 4 random images of different variables arranged in 2 columns.
Each rater received the catalog and an evaluation sheet with a 100-mm VAS. On the VAS, the leftmost position indicated "very unattractive" and the rightmost position "very attractive." The VAS score ranged from 0 to 100, with 0 being the minimum and 100 the maximum esthetic value. The raters were instructed to not compare smiles in the album. The scores were measured from the leftmost point to the mark made by the rater. One researcher (S.M.A.) measured the length using an electronic digital caliper. All values obtained in millimeters were registered as scores.
The data were statistically analyzed with PASW Statistics software (version 18.0; IBM Co., Armonk, NY, USA). Descriptive statistics are reported as means and standard deviations. Differences in the mean esthetic scores among the levels of asymmetries were analyzed by using a one-way repeated analysis of variance (ANOVA). The hypothesis that there was no difference between the various altered smiles among each group of raters was tested. Newman-Keuls multiple comparisons were conducted as post hoc analyses. The level of significance was established as 5%. Furthermore, the distribution of the mean scores was compared among the three groups.

RESULTS
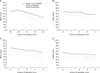
Means, standard deviations, and the result of the Newman-Keuls test for each group are shown in Figure 5 and Tables 1,2,3,4. In the most altered photograph for each variable, the VAS scores were significantly different among the three groups.
The VAS scores of group 3 (F = 43.41; p < 0.0001) were significantly lower when the gingival margin height of the central incisor was changed 1.0 mm or more. The VAS scores of group 1 (F = 18.60; p < 0.0001) and group 2 (F = 16.65; p < 0.0001) were significantly lower when the gingival margin height of the central incisor was changed 1.5 mm or more (Table 1).
Regarding the lateral incisor crown width and length, the VAS scores of group 3 (F = 9.78; p < 0.0001) were significantly lower for changes of 3.0 mm or greater. Similarly, group 1 (F = 4.04; p = 0.0003) and group 2 (F = 10.46; p < 0.0001) could distinguish a 3.0-mm change in crown width, although each group showed overlapping of the Newman-Keuls groups for 2 photographs (the 1.0-mm and 2.0-mm altered photographs in group 1 and the 2.0-mm and 3.0-mm altered photographs in group 2) (Table 2).
The VAS scores of group 3 (F = 21.40; p < 0.0001) were significantly lower when the canting of the incisal plane was 1.0 mm, while they were lower in group 2 (F = 16.90; p < 0.0001) when the canting was 2.0 mm. Group 1 (F = 6.83; p < 0.0001) perceived a change when the amount of canting was 3.0 mm or greater, although the Newman-Keuls groups overlapped for 2 photographs (the 1.0-mm and 2.0-mm altered photographs) (Table 3).
Group 1 (F = 1.41; p = 0.23) showed no significant difference among all photographs with dental midline shifts, unlike group 2 (F = 4.62; p = 0.001) and group 3 (F = 3.72; p = 0.006), which showed significantly different VAS scores and demonstrated overlap of the Newman-Keuls groups for 2 photographs (the 2.0-mm and 3.0-mm altered photographs in both groups). Both groups perceived a change when the amount of shift was 3.0 mm or greater (Table 4).
When the perceptive ability among the three groups was compared, statistical differences in most situations were observed. However, no difference was shown among the three groups in perceiving the original image versus an image in which the central incisor gingival margin height had been altered by 0.5 mm. Group 3 showed lower scores than the other groups. Groups 1 and 2 showed differences in perceiving the image in which the incisal plane was canted 4.0 mm and the dental midline was shifted 3.0 mm (Tables 1,2,3,4).
Regarding gender, there was no statistically significant difference in the reported VAS scores (p < 0.05).
DISCUSSION
In order to investigate the effects of orthodontic treatment experience on one's perception of smile esthetics, we used four variables in this study: maxillary central incisor gingival margin height, maxillary lateral incisor crown width and length, canting of the incisal plane, and dental midline shift. Although other various factors affect the smile, these four variables are easy to perceive and showed differences between laypersons and dentists in other studies.4,5
In most situations, dentists were more critical of dental esthetics than laypersons (Tables 1,2,3,4). This finding corroborates the results of previous studies regarding esthetic perceptions showing that dentists and laypersons have different perceptions of smile esthetics and that dentists are less tolerant of some dental conditions than the general public.4,5,19,20,21,22
Recent studies reported that laypersons could not detect an asymmetric crown length unless 1 crown was 1.5-2.0 mm shorter than the other.5,22 Similarly, in our study, the non-treated group perceived a smile as unattractive when the gingival margin height was 1.5 mm or greater, while the dentist group perceived it as such when the margin height was 1.0 mm or greater (Table 1). This suggests that correcting gingival margin asymmetries of the maxillary central incisors in the range between 0.5 mm and 1.5 mm might be not necessary, since it is not a concern of patients.23,24 However, correcting such an asymmetry might be justifiable after it is fully discussed with the patient.
In clinical situations, we frequently encounter patients with a lateral incisor that is shorter or narrower than the contralateral incisor. In this study, the dentist group perceived a smile as unattractive when the crown width difference between the maxillary lateral incisors was 3.0 mm (Table 2). This result in the dentist group was the same as in the study of Kokich et al.,5 but the results from the layperson (non-treated) group showed some differences. In their study, the layperson group perceived a 4.0-mm discrepancy; but in our study, the non-treated group could not perceive such a minor change. They also reported that it was difficult for laypersons to perceive change when the crown length was decreased along with the crown width (4.0 mm) while maintaining the same ratio, and more difficult than when only the crown width was decreased (2.0 mm). In this study, unlike the non-treated group, the treated group was able to distinguish between a 1.0-2.0 mm change and a change of 4.0 mm, meaning that the perceptive ability of the treated group to distinguish changes was greater than in the non-treated group (Table 2).
In this study, the dentist group perceived a smile as unattractive when the canting of the incisal plane was 1.0 mm. The treated and non-treated groups perceived it as unattractive when the cantings were 2.0 mm and 3.0 mm, respectively (Table 3). These results are similar to those of Kokich et al.,4 who reported that the threshold was 1.0 mm among orthodontists and general dentists, while it was 3.0 mm among laypersons. Ker et al.25 also found that laypersons accepted as much as 4 degrees of canting (equivalent to 3.0 mm). However, there was no report regarding the increased perceptive ability of a treated group. The threshold difference among dentists, treated laypersons, and non-treated laypersons in our study could mean that the experience of orthodontic treatment affects perceptive ability regarding incisal plane canting. In contrast, Padwa et al.26 reported that the perception of occlusal plane canting depends on the degree of inclination, and not necessarily on the levels of experience of the observers.
The dentist group perceived a difference when the midline was shifted 3.0 mm in this study (Table 4). Similarly, Kokich et al.4 reported that orthodontists classified smiles as least attractive only when midline shifts reached 4.0 mm. On the contrary, Pinho et al.22 reported that orthodontists and prosthodontists were less tolerant of dental midline shifts, and rated 1.0 mm and 3.0 mm shifts as less attractive, respectively. The non-treated layperson group could not perceive dental midline shifts in this study, similar to the results of other studies.4,22 However, some studies reported that midline shifts greater than 2.0 mm are perceived by most people,20 and 56% of laypersons noticed 2.0-mm midline shifts.21 Moreover, Ker et al.25 reported that maxillary and mandibular dental midline deviations were deemed acceptable by laypersons until they exceeded 2.9 mm and 2.1 mm, respectively. These differing results can be explained by the different digital alterations, specialist participants, statistical analyses, and questionnaires. In these studies, only the maxillary or mandibular dental midline was shifted in the facial photographs, including the eyes and nose. Moreover, laypersons evaluated the photographs only as "acceptable" or "not acceptable" and did not score them. Our study is notable because the perceptions of dental midline shift were similar between the treated group and the dentist group. This finding is different from another study18 concluding that orthodontic treatment experience did not influence a layperson's perception of maxillary dental midline shifts. These discrepant results might be explained by differences in the methods used, and by the degrees and numbers of image alterations. Based on this result, we speculate that a patient's esthetic perception is improved through orthodontic treatment because of the increased attention paid during frequent appointments with an orthodontist.
Previous studies regarding the influence of age on esthetic perceptions showed discrepant findings.1,10,12,27 Some studies reported that young adults paid more attention to the appearance of anterior teeth,12,27 while other studies reported that age did not influence esthetic perceptions.1,10 Therefore, we restricted the age range of the laypersons to exclude the influence of age from this study. The male-to-female ratio in our study was 12:38 for non-treated laypersons, 6:44 for treated laypersons, and 17:13 for dentists, respectively. There was no statistically significant difference in the mean scores given by men and women raters within each group. This agreed with the findings of Kokich et al.5 and Rosenstiel and Rashid,6 but is in contrast to the findings of Geron and Atalia,8 where women were found to be more tolerant of upper gingival exposure. This difference in results between the two studies is likely attributable to variations in esthetic perceptions among different populations.
In order to simulate smile esthetics, we used a computer program to produce various dental conditions in this study. It was possible to assess various dental features independently using the same photograph. In our study, laypersons with orthodontic treatment experience showed more keen perceptive abilities than those without treatment experience. However, we are not suggesting that the results of our research should be interpreted as a general fact that can be applied to every patient in practice.
This study was a cross-sectional study with different participants included in the non-treated and treated groups. Therefore, a longitudinal study using the same participants in a non-treated group before treatment and in a treated group after treatment should be conducted in order to confirm whether orthodontic treatment experience affects perceptions.
CONCLUSION
To examine whether the experience of orthodontic treatment affects the individual's perception of smile esthetics, computerized image alterations and questionnaires with a VAS were used to compare perceptions among laypersons with and without orthodontic treatment experience and dentists.
Laypersons with and without orthodontic treatment experience and dentists had different perceptions of smile esthetics. While laypersons perceived a 1.5 mm decrease in the gingival margin height of the maxillary central incisor, dentists perceived a 1.0 mm decrease. Laypersons and dentists classified smiles as least attractive when alterations of the crown width and length of the maxillary lateral incisor reached 3.0 mm. Non-treated laypersons perceived changes in the incisal plane when the canting was 3.0 mm, while treated laypersons and dentists perceived canting at 2.0 mm and 1.0 mm, respectively. Dental midline shifts were perceived at 3.0 mm by treated laypersons and dentists.
The results of the present study suggest that orthodontic treatment experience improved esthetic perceptions among laypersons.








 XML Download
XML Download