

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Facial esthetics has become increasingly important in the orthodontic field as an increasing number of patients are seeking orthodontic treatment not for better masticatory function and stability alone but also for aesthetic concerns. Moreover, besides being concerned about lip protrusion and dental crowding, they are also interested in addressing maxillofacial deformities.
Skeletal deformity manifests in three planes: vertical, horizontal, and anteroposterior. Maxillofacial deformity, including facial asymmetry, is associated with vertical andanteroposterior involvements. For instance, at least 21-67% of patients with mandibular prognathism or retrognathism present with facial asymmetry.1,2 Facial deformation has drawn attention in orthodontics and in oral and maxillofacial surgery for a long time because it requires maxillofacial correction, which may involve orthognathic surgery.
A postural deformity of the trunk such as idiopathic scoliosis can affect occlusion. Adolescents with congenital hip dislocation often present with asymmetric occlusion and are more prone to developing crossbite.3 Patients with Duchenne muscular dystrophy present with posterior enlargement of the mandible arch and development of Class III malocclusion.4
Scoliosis presents as a two-dimensional spinal deformity in the coronal plane. In reality, however, scoliosis is a three-dimensional involvement with loss of normal curvature in the sagittal plane along with a vertebral rotational deformity in the coronal plane. Various classifications of idiopathic scoliosis have been discussed; however, consensus on the most appropriate classification has not yet been reached.5
Analyzing the facial form of scoliosis patients in the frontal plane alone has limited value.1,2 Therefore, it is meaningful to investigate the anteroposterior and vertical relationships for an analysis of the facial form in scoliosis patients.
Previous studies on idiopathic scoliosis and the facial skeleton have reported that idiopathic scoliosis and facial asymmetry are related.6,7 However, the degree of the curvature, and the number and location of these curves were not considered in the analyses.
Since idiopathic scoliosis is a complex three-dimensional deformity, and only one particular plane cannot reveal the full extent of the scoliosis, the severity, location, and number of curves should be considered rather than following the conventional methods of measuring the deformity in idiopathic scoliosis. These combined analyses may provide a way to enhance our understanding of the relationships between scoliosis and facial deformities. Therefore, this study aimed to evaluate the following null hypothesis: Idiopathic scoliosis and facial deformity in horizontal, vertical, and anteroposterior planes are related, and facial deformities are directly proportional to the severity of scoliosis.
Go to : 
MATERIALS AND METHODS
Subjects
A total of 123 female patients aged 14 years or older who visited the Spine Clinic at the Department of Orthopedics, Korea University Guro Hospital (Seoul, Korea) for treatment of idiopathic scoliosis and had no previous orthodontic treatment were enrolled in the study. This study was approved by the institutional review board of Korea University Guro Hospital (KUGH10235) and written informed consent was obtained from the patients. Whole-spine standing anteroposterior and lateral radiographs and lateral and frontal cephalograms were obtained for this study. Female patients under the age of 14 years and male patients were excluded because of expected changes in facial form and cephalometric measurements with continuing growth. As female patients aged less than 14 years have not crossed the adolescent growth spurt and male patients can grow for a long time at adolescence, there is a potential for facial bone growth and facial form changes. Consequently, only female patients aged 14-28.5 years (average, 15.9 years) were included in this study.
Radiographic measurements and classification of scoliosis
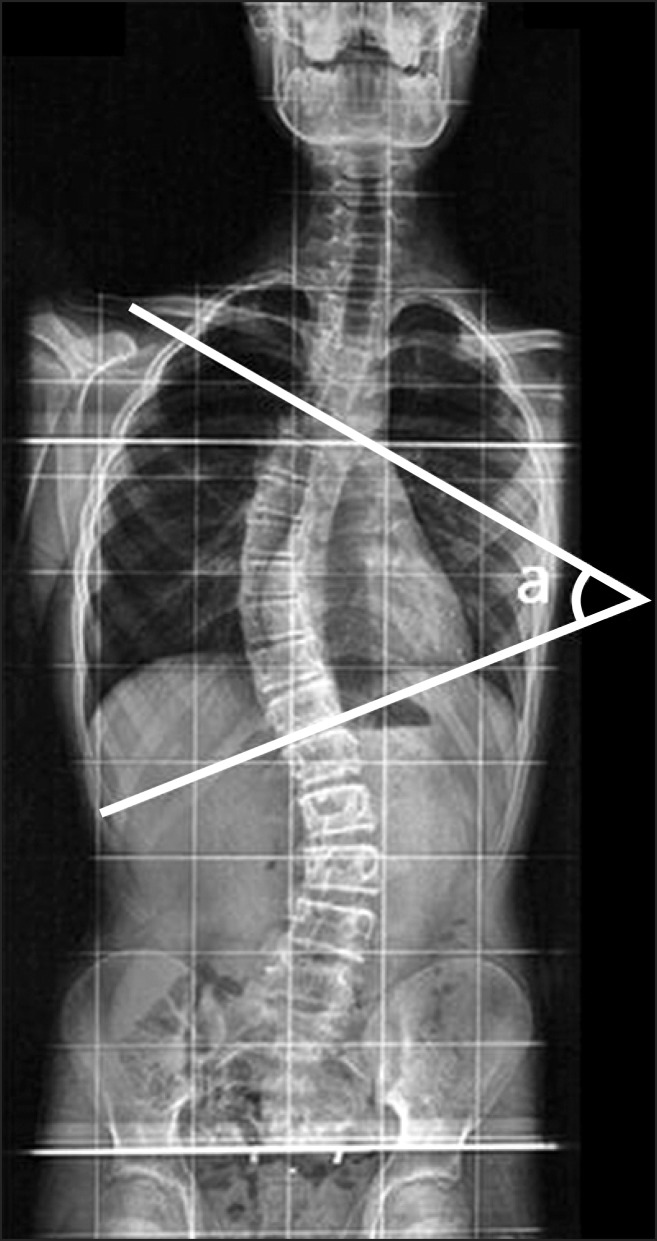
Whole-spine anteroposterior and lateral radiographs were taken with the patient in a naturally erect position with the use of a horizontal reference line (HRL) and a vertical reference line (VRL), which were defined as a line parallel to the floor and a line perpendicular to HRL, respectively. Scoliosis was classified according to two methods, the Cobb angle and the Lenke classification of six curves (Table 1). Measurements and re-measurements (one month later) were performed using the PiViewSTAR software (Infinitt, Seoul, Korea) by the same orthopedic surgeon. In the intraobserver analysis, the intraclass correlation coefficient (ICC) was 0.985 (p < 0.001).

Classification according to the Cobb angle
Cobb angle (Figure 1) is the angle between a line drawn parallel to the superior end-plate of the top vertebra of the curve and a line drawn parallel to the inferior end-plate of the bottom vertebra of the curve. Although Cobb angle is usually classified into four groups (normal, mild, moderate, severe), the normal group (Cobb angle < 10°) was excluded from the classification in this study: mild (Cobb angle 10-25°), moderate (Cobb angle 25-40°), and severe (Cobb angle > 40°). The orientation of the vertebral curve was identified as right or left based on the location of the main curve.
The Lenke classification of six curve types
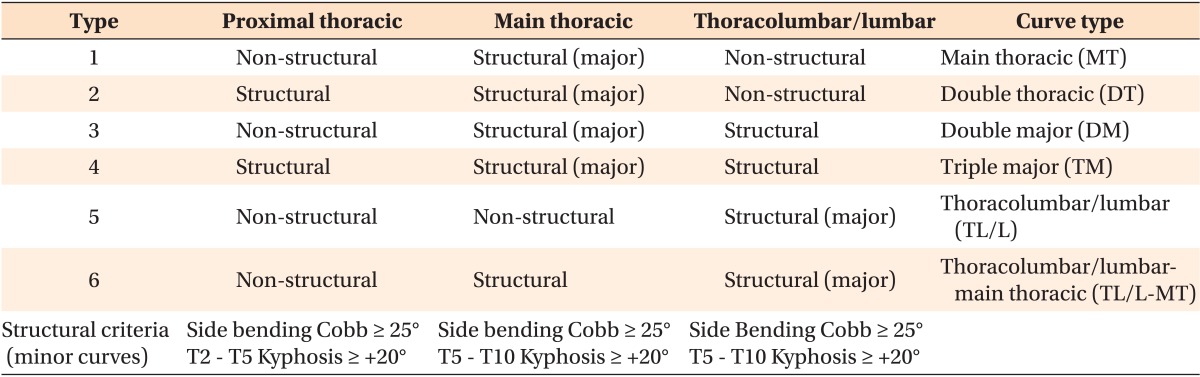
Scoliosis is classified into six curve types according to the structural characteristics of the major and minor curves.8 A Cobb measurement is obtained, and the curves are classified as major or minor with the largest numerical curve being designated the major curve. Based on his classification scheme, only thoracic and thoracolumbar/lumbar curves can be the major curve. A curve is denoted as structural if the side bending Cobb angle is at least 25° or if the kyphosis is at least 20°. When the major and minor curve patterns are combined, six curve types emerge and can be identified as curve types 1-6, as shown in Table 2.
Frontal cephalograms
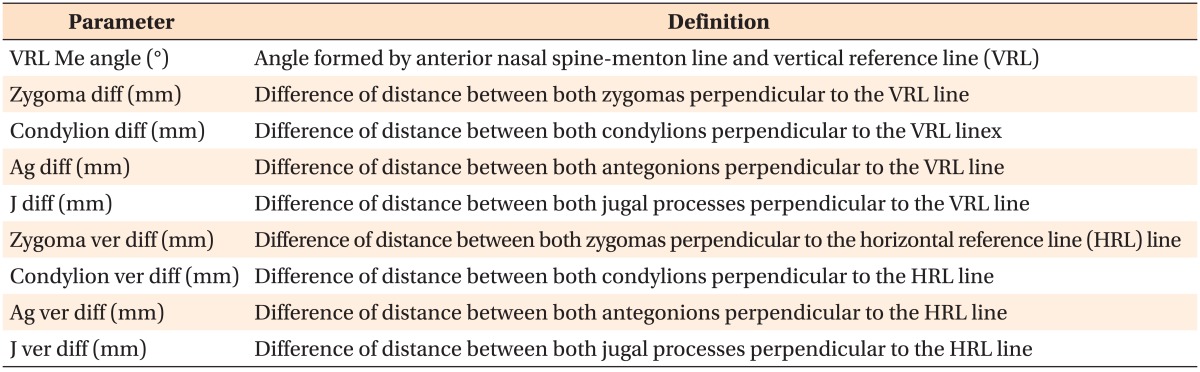
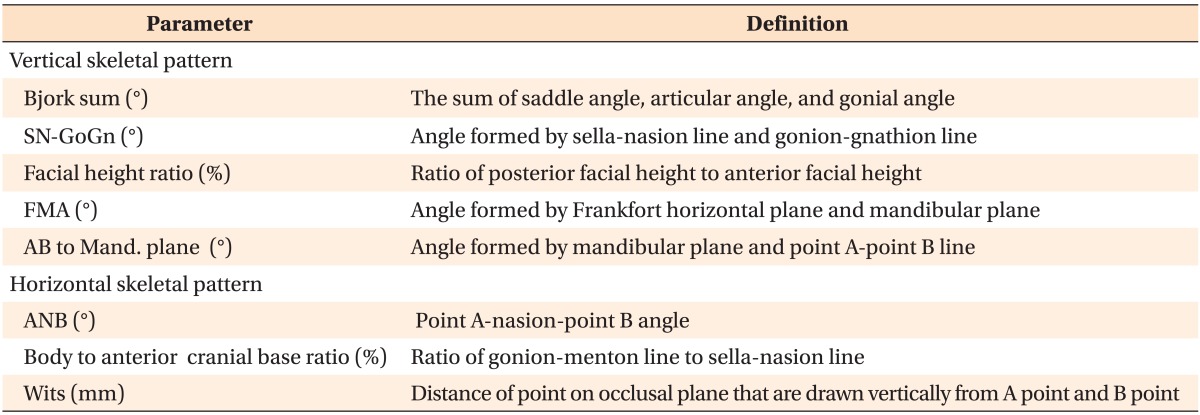
A frontal cephalogram is taken with teeth in habitual maximum intercuspation and in an erect position with the Frankfort horizontal line parallel to the floor and patient's head fastened with an ear rod. Cephalometric analysis was mainly performed using landmarks related to facial asymmetry. HRL was defined as a line connecting the right lateral orbitale (Lo) and left Lo. VRL was defined as a perpendicular bisector of right and left Lo.9,10,11 Tracing was carried out twice in an interval of one month with V-Ceph 5.5 (Cybermed, Seoul, Korea) by one orthodontist. The ICC used to determine the intraobserver error was 0.990 (p < 0.001). Cephalometric landmarks, parameters, and reference lines are shown in Table 3 and Figure 2.
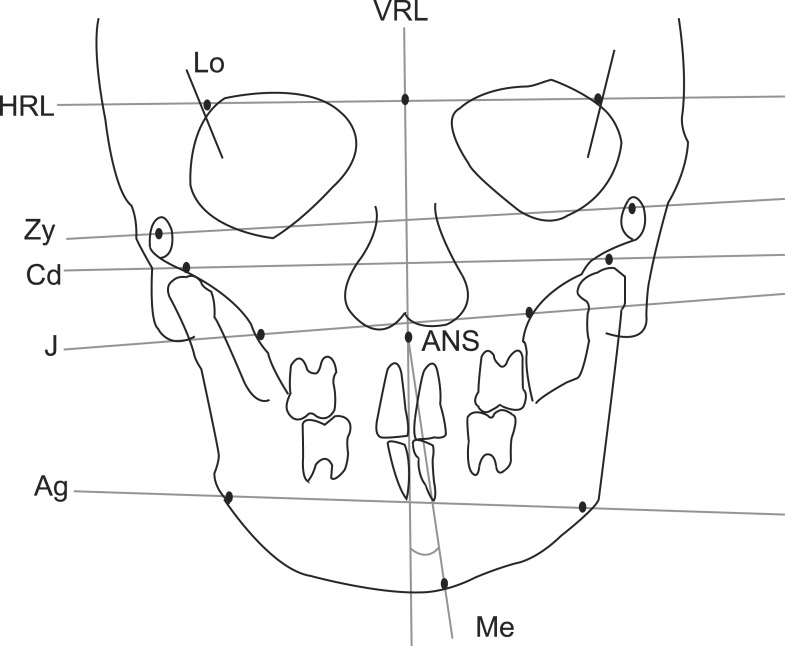
The left deviation of the measurements was set as negative numbers and the right was set as positive numbers for each parameter. Parameters defined by the difference between the left and right values were measured by subtracting the right value from the left.
Lateral cephalograms
Cephalometric analysis of lateral cephalograms was conducted with landmarks that are often used for general diagnostic purposes. Each cephalogram was classified as having a vertical or horizontal skeletal pattern according to its characteristics. The same tracing protocol as the one used in the frontal cephalometric analysis was followed. One orthodontist performed the cephalometric tracing twice in an interval of one month with V-Ceph 5.5 (Cybermed, Seoul, Korea). The ICC used to determine the intraobserver error was 0.999 (p < 0.001). Cephalometric landmarks, parameters, and reference lines are shown in Table 4 and Figure 3.

Statistical analysis
The Kruskal-Wallis test was performed to investigate the relation between each of the idiopathic scoliosis groups and cephalometric measurements of frontal and lateral cephalograms. Statistical analysis was carried out with SPSS software ver. 12.0 (SPSS, Chicago, IL, USA) with a significance level of p < 0.05.
Go to :
RESULTS
Cobb angle
The 123 subjects were classified according to their Cobb angle into 3 groups: mild (n = 26), moderate (n = 56), and severe (n = 41).
For the frontal cephalogram, which is in the same coronal plane as the vertebral curve, the results were divided into left and right following the direction of the vertebral curve (the location of the apex) (Table 5). The parameters showing the left and right difference in the facial form had no relation with the direction of the vertebral curve. Facial asymmetry was not significantly related to the scoliosis severity.
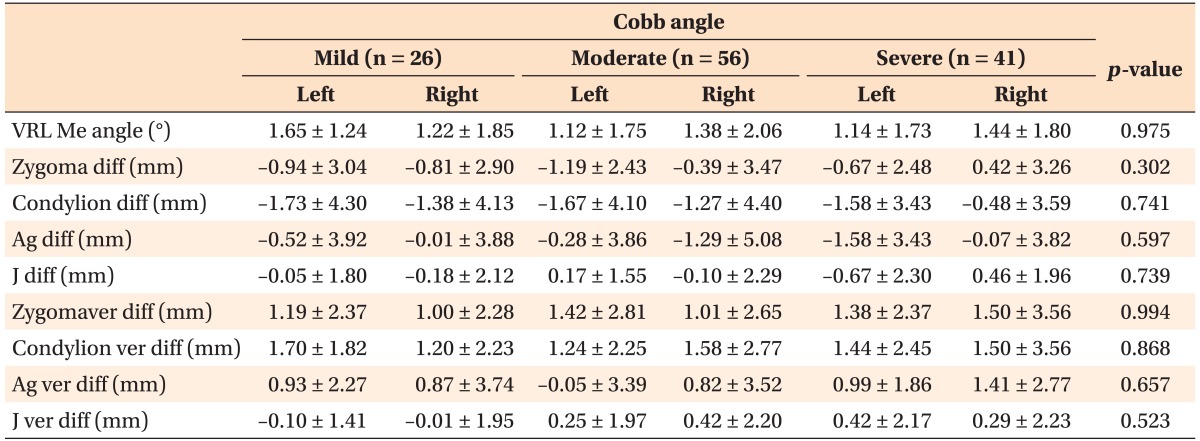
Table 5
Comparison of frontal cephalometric measurements according to the Cobb angle
Values are presented as mean ± standard deviation.
Kruskal-Wallis test was performed.
Definition of each parameter is described in Table 3.
![]()
In the lateral cephalometric measurements (Table 6), the vertical and horizontal skeletal pattern parameters had no significant difference among the groups.
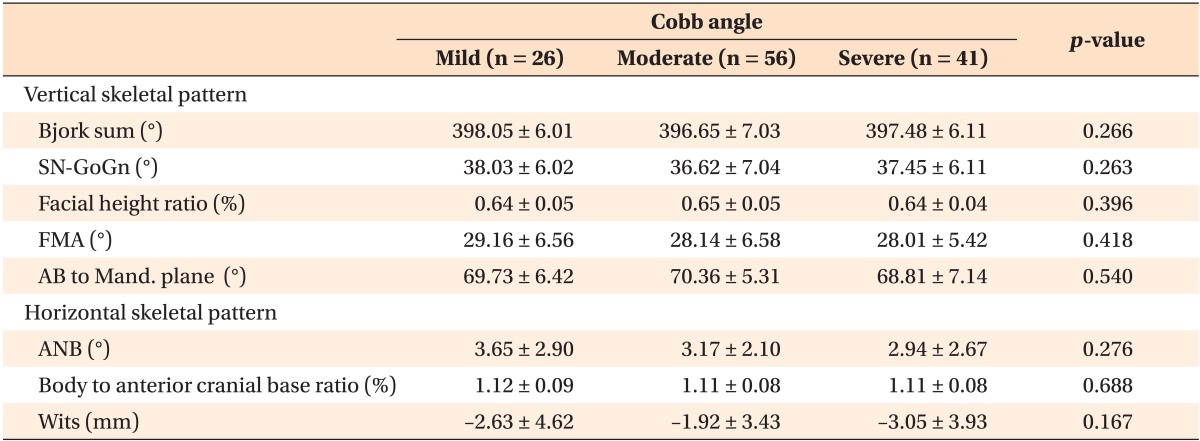
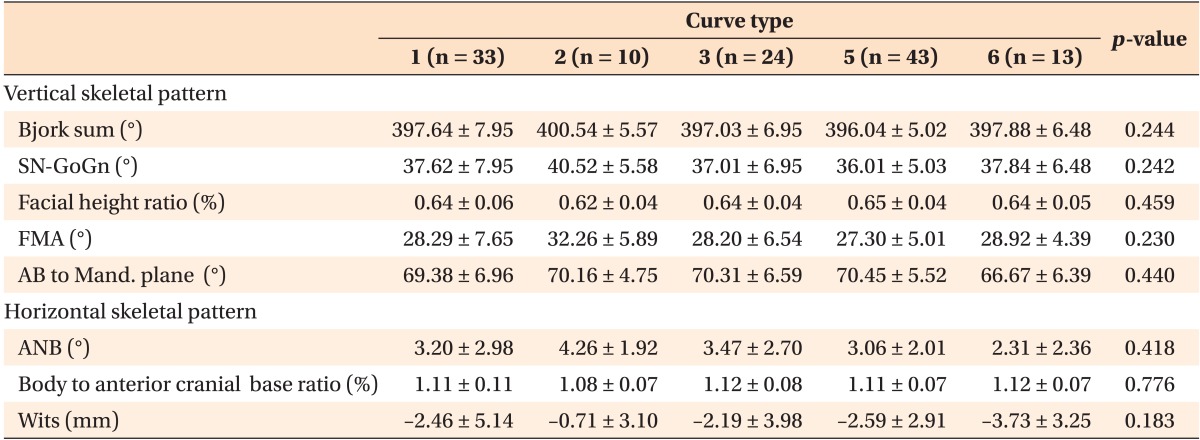
Table 6
Comparison of lateral cephalometric measurements according to the Cobb angle
Values are presented as mean ± standard deviation.
Kruskal-Wallis test was performed.
Definition of each parameter is described in Table 4.
![]()
Curve types of the Lenke classification
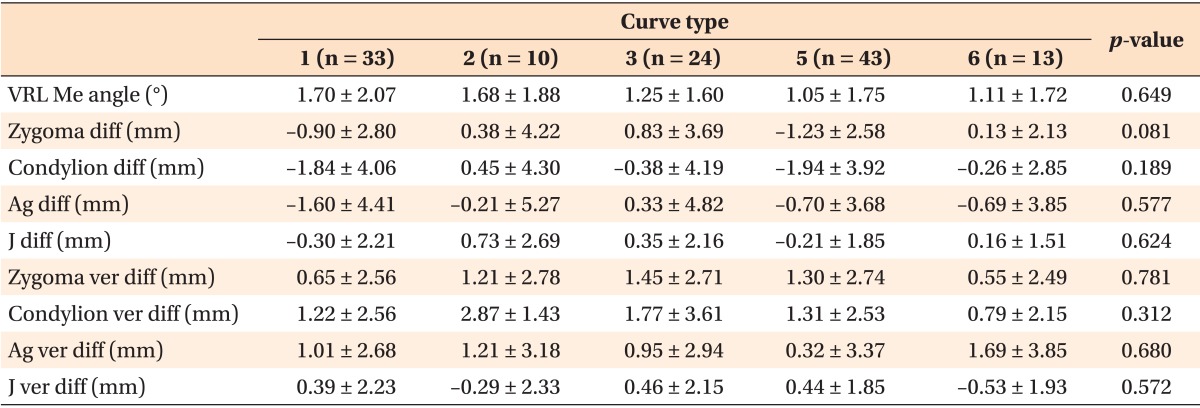
The location and number of vertebral curves are divided into six groups according to the Lenke classification. Among 123 subjects, 33 were type 1, 10 were type 2, 24 were type 3, 43 were type 5, and 13 were type 6.
The parameters of facial asymmetry from the frontal cephalometric measurements were not related with the curve types based on the Lenke classification. Since Lenke classification is based on the location and the number of the vertebral curves, we can reasonably infer that facial asymmetric parameters were not related with the location and number of vertebral curves (Table 7).
In lateral cephalometric measurements, vertical and horizontal skeletal patterns were not related among the groups (Table 8).
Go to :
DISCUSSION
Correlation between facial form and head posture has been examined based on radiographic measurement in a previous study.12,13 It was reported that patients with a long face tended to have longer and straighter cervical vertebrae, whereas those with a short face have more curved cervical vertebrae.13 Another study has reported an association between head posture against cervical vertebra and the vertical relationship of the mandible due to a differential growth of the muscles and fascia which are attached to the mandible.14,15 Solow and Sandham16 identified an association between head posture and craniofacial morphology. Upper airway obstruction due to disease and neuromuscular feedback lead to an extension of the head with change in the craniocervical angle, which in turn brings about soft tissue stretching affecting the skeleton and eventually resulting in a morphological change in the head.
A relationship between the facial morphological change and deformation of other body parts, and an association between malocclusion and head posture or deformation of the body has been reported. Solow and Sonnesen13 reported an association between anterior crowding and craniocervical posture based on oral examination and a lateral cephalogram. They found that in patients with anterior crowding of 2 mm or more in the maxilla or mandible, the craniocervical angle was on an average greater by 3-5°. They also observed a similar correlation in Class II malocclusion patients. On the contrary, the coronal curvature of thoracic and lumbar vertebrae was not associated with indicators of the horizontal skeletal pattern of the skull in the sagittal plane in this study. This result was similar to that of a study by Motoyoshi et al.17 on the effect of head posture on occlusion using finite element analysis.
Ben-Bassat et al.18 reported that malocclusion characteristics were associated with asymmetry in patients with idiopathic scoliosis. They found a predominence of subdivision was evident among the patients with scoliosis (21.9%) compared with the control group (8.5%) in Class II malocclusion, midline deviation, and crossbite in scoliosis patients. Harila et al.3 reported that the incidence of crossbite was higher in patients with congenital hip joint displacement than in a healthy population. They argued that general postural deformity leads to asymmetric development of occlusion and crossbite. However, these two studies were conducted on the basis of an oral examination and study model without cephalometric analysis, and only dental malocclusion was evaluated. In comparison with the traditional diagnostic process for malocclusion or facial asymmetry, skeletal problems were not properly investigated.
Association between facial asymmetry, shoulder imbalance, and scoliosis was reported in a study by Hong et al.19 They found a statistically significant correlation between anterior nasal spine (ANS)-menton angle and Cobb angle in the frontal cephalogram and identified a relationship between facial asymmetry and scoliosis, which was contrary to the results of this study. Although ANS-menton angle is one of the cephalometric measurements used for diagnosis of asymmetry in the frontal cephalogram, ANS-menton angle alone is not sufficient for an evaluation of asymmetry because of the variation in ANS.9,10,11 Besides this, no relationship was found with other cephalometric measures of asymmetry. In addition, the sample size of this study was small (n = 69), and the growth potential was not excluded as male patients were also included, and the average patient age was 13.7 years.
Saccucci et al.20 and Segatto et al.21 reported that scoliosis has a strong relationship with malocclusion and facial asymmetry. The patients with idiopathic scoliosis showed a high prevalence of facial asymmetry like unilateral Class II malocclusion, upper and lower midline deviation, and unilateral crossbite. In these reports, the results were compared with the control group (patients without idiopathic scoliosis), which were evaluated in the coronal and sagittal planes. Korbmacher et al.22 reported a significant association between crossbite and scoliosis with respect to the normal conrol group but did not show a relationship between scoliosis and the direction of the vertebral curve; this was in agreement with the results of our study. However, in previous studies, facial asymmetry and scoliosis were not found to be related with regard to the severity of the scoliosis and the location and number of vertebral curves.
In most of the previous studies that evaluated the relationship between facial asymmetry or malocclusion and idiopathic scoliosis, scoliosis was classified using the Cobb angle. Use of Cobb angle alone for classification of scoliosis has limitations. Of the various classifications introduced so far, the Kong-Moe classification suggested by King et al.23 is the most popular. However, several limitations of this classification have been highlighted. First, it only deals with the thoracic vertebral curve and does not describe the isolated thoracolumbar and lumbar curves and the triple major curves. Intraobserver and inter-observer error is also relatively high with poor-to-fair validity, reliability, and reproducibility. In addition, the deformities are evaluated only in the coronal plane, failing to assess the sagittal planes.24,25 In response to these shortcomings, Lenke et al.26 developed a more objective and comprehensive classification system. This classification provided an assessment in the sagittal plane and enabled determining the degree and complexity of the curve. It also addressed the lumbar curve, which can cause coronal decompensation and provided a detailed description of the classification criteria. In these respects, this scheme is considered a more advanced classification system.27,28 In this study, idiopathic scoliosis was classified in further detail with the Lenke classification system, and the Cobb angle classification was also provided for a comparison with previous studies.
In this study, we found that idiopathic scoliosis and facial form variations are not related, which is in contrast to previous literature29,30 that reported facial form variation such as Class II malocclusion or lateral crossbite in scoliosis patients. Certain compensatory mechanisms may have minimized the effects of scoliosis on the maxillofacial area during growth.
Limitations of this study include evaluation of only female patients and an insufficient sample size (n = 123) for performance of parametric statistics; further studies are therefore required to address these limitations.
Go to :
CONCLUSION
This study investigated for possible associations between idiopathic scoliosis patients classified according to Cobb angle (mild, moderate, and severe) and curve type (type 1-6) of the Lenke classification and their facial forms analyzed in horizontal, vertical, and anteroposterior planes from cephalometric measurements. The null hypothesis was rejected because occurrence of facial form deviations are not increased in proportion to the severity of scoliosis. Based on the results of this study, no apparent relation was observed between the severity of scoliosis and facial form variations in idiopathic scoliosis patients.
Go to :
 XML Download
XML Download