

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Anchorage control is essential for a good outcome in extraction cases. The most challenging situation is to achieve en-masse retraction with minimal or no anchorage loss.1,2 Conventional anchorage techniques include headgears, transpalatal arches, and Nance buttons combined with full-arch bonding. More recently, temporary skeletal anchorage devices (TSADs) were introduced for biomechanical therapy.3,4,5,6,7 TSADs are commonly used in contemporary orthodontics, but can exhibit failure and weakness when multidirectional or heavy forces are applied.
In many cases of dentoalveolar protrusion, patients have Class I molar relationships with good interdigitation of the posterior teeth. Once brackets are bonded, the occlusion is inevitably altered and requires further correction. The periodontal challenge to posterior teeth should also not be overlooked. In 2007, Chung et al.8 proposed an approach to TSAD-dependent en-masse retraction (biocreative orthodontics). In their protocol, the maxillary anterior teeth are retracted en-masse, but no orthodontic appliances are attached to the posterior teeth during retraction.8,9 This concept evolved after the development of the C-implant, because a partially osseointegrated mini-implant or miniplate can easily endure multidirectional or heavy forces applied by archwires and springs.7,8,9,10,11
Although the biocreative therapy using conventional C-wires has many advantages, such as low friction, reduced periodontal challenges to the posterior teeth, and no impact on normal posterior occlusions, extra training regarding the placement of steps and bends in the stainless steel (SS) archwires may be required of clinicians to properly engage crowded and unleveled anterior teeth (Figure 1A and 1B).12,13 The high load-deflection rate of conventional C-wires necessitates regular and sometimes tedious archwire adjustments at each visit, increasing chairside time. To overcome these shortcomings, we designed a preformed assembly of nickel-titanium (NiTi) and SS archwires (preformed C-wire; Figure 1C and 1D).
The aim of this retrospective study was to evaluate the therapeutic effects of preformed C-wires combined with TSADs as the sole source of anchorage and to compare these effects against those of conventional C-wires for en-masse retraction. The null hypothesis was that the two archwire systems would show no differences in therapeutic effects.
MATERIALS AND METHODS
Patients
Thirty-one female patients with skeletal Class I or II dentoalveolar protrusion, mild-to-moderate anterior crowding (3.0-6.0 mm), and stable Class I posterior occlusions were divided into conventional C-wire (n = 15; mean age = 20.0 ± 3.3 years) and preformed C-wire (n = 16; mean age = 21.5 ± 3.6 years) groups. The patients underwent extraction of all the first premolars. Then, one orthodontist (J.J.H) retracted the maxillary anterior teeth en-masse using 0.022-inch-slot preadjusted edgewise anterior brackets, the assigned C-wire, and maxillary TSADs; no appliances were bonded to the maxillary posterior teeth during retraction. The retraction distance and number of clinical visits were controlled between groups. This study was reviewed and approved by the Institutional Review Board of The Catholic University of Korea, Seoul St. Mary's Hospital (KIRB-00384-20-008).
Maxillary appliances
Two-component C-implants (Cimplant Co., Seoul, Korea) or C-tubes (Jin Biomed Co., Bucheon, Korea) were used for direct anchorage (Figure 2). The C-implant (1.8 mm in diameter and 8.5 mm in length) is a sandblasted, large-grit, acid-etched mini-implant. The C-tube is a miniplate with an extended arm that includes an adjustable tube to accept a wire. The TSADs were placed at the beginning of the treatment for simultaneous leveling and space closure. The C-implants were placed in the maxillary interseptal bone between the second premolars and the first molars bilaterally. If C-tubes were used, the fixation screws were located more apically, and the heads of C-tubes were placed in the same vertical level as that of C-implants.
Preformed C-wires have two components, as shown in Figure 3. One component is the NiTi archwire, designed to engage the maxillary anterior teeth (canine to canine). In this study, we used 0.016 × 0.022-inch superelastic NiTi archwires without built in torque (BioTorque; Forestadent Bernhard Förster GmbH, Pforzheim, Germany), which can be easily ligated to crowded teeth. The other component consisted of 0.017 × 0.025-inch SS archwires with retraction hooks. Furthermore, 0.022-inch crimpable inside diameter tubes were soldered to the SS archwire and the NiTi archwire was inserted into the tubes. We positioned the tubes on the NiTi archwire between the lateral incisors and the canines bilaterally and crimped them firmly in place. The SS archwire was then inserted into the TSADs, creating a rigid sliding section with a built in power arm. The archwire did not need to be bent for vertical correction of high canines during retraction. During the initial alignment, 2.5-oz elastics or elastic chains delivering 0.7 N of force were applied to the canines. The canines were retracted while the incisors were aligned. Once all the anterior teeth were aligned with the archwire, closed-coil NiTi springs (1.2 N) or 4.5-oz elastics were used for en-masse retraction.
Mandibular appliances
Bonded mesh-tube appliances (BMTAs), comprising 0.022-inch buccal tubes on the mandibular second premolars and metal mesh on the mandibular first molars, were used bilaterally for anchorage reinforcement and maintenance of normal posterior occlusion in the preformed C-wire group (Figure 4). During leveling, 0.018-inch reverse curve NiTi archwires and Class III elastics attached to the TSADs were used to prevent mesial tipping of the mandibular molars. During retraction, bilateral Class I elastics were used between the canines and the hooks of the BMTAs. After space closure, short-term fixed appliances, tooth positioners, or clear aligners were used for finishing. In the conventional C-wire group, conventional brackets were bonded to the mandibular dentition and space closure was performed with power chains.
Data collection
Lateral cephalograms were obtained before treatment (pretreatment) and after space closure (post-retraction). Soft tissue, skeletal, and dental variables were measured as previously described (Figures 5 and 6).11 In particular, lip protrusion, vertical or horizontal skeletal pattern, and positional changes of the first molars and central incisors were assessed.
Statistics
The means and standard deviations of 19 cephalometric variables were calculated. To evaluate tracing and measurement errors, all variables were re-measured after 3 weeks. Agreement was quantified by calculating intraclass correlation coefficients (ICCs); ICCs greater than 0.95 indicated reliable measurements. Normal distribution was confirmed by using the Shapiro-Wilk test (p > 0.05). Intragroup pretreatment and post-retraction data were compared using the paired t-test, and the pretreatment data and amount of change between the groups were analyzed with the independent t-test. p < 0.05 was used to indicate a significant difference.
RESULTS
Figures 7, 8 and 9 depict progress from the beginning of treatment to space closure in a 23-yr-old patient from the preformed C-wire group; her chief complaint was protrusive lips and crowded teeth. We used C-tubes designed for SS archwire insertion in the maxillary posterior region to achieve direct skeletal anchorage. Mandibular anchorage was reinforced with the BMTAs during retraction. Crowding was controlled along with retraction of the maxillary anterior teeth.
No failure of the TSADs was observed in either group during treatment. In the conventional C-wire group, the mean retraction period was 13.44 ± 4.30 months and the mean overall treatment time was 23.45 ± 4.31 months; these periods were shortened by 3.2 and 2.5 months, respectively, in the preformed C-wire group.
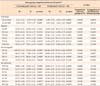
The groups did not show significant differences in anteroposterior and vertical skeletal patterns and inclination of anterior teeth before treatment (Table 1), except LC-L6 (p < 0.01, data not shown). The maxillary anterior teeth were fully retracted to close the extraction spaces (PTV-U1, p < 0.001 for both groups). Uprighting of the maxillary anterior teeth by controlled tipping was observed (SN-U1: p < 0.001 for the conventional C-wire group; p < 0.01 for the preformed C-wire group). The maxillary molars in the preformed C-wire group showed no significant mesialization, mesial tipping, or extrusion. However, some mesialization and mesial tipping of the maxillary molars was observed in the conventional C-wire group (PTV-U6, p < 0.001; SN-U6, p < 0.05). Linguoversion of the mandibular anterior teeth was obvious in both groups (MP-L1, p < 0.001), but mesialization and mesial tipping of the mandibular molars were significant only in the conventional C-wire group (MP-L6, p < 0.01; LC-L6, p < 0.001). Furthermore, slight extrusion of the mandibular teeth was observed in both groups (MP-L1v and MP-L6v, p < 0.01 for the conventional C-wire group; MP-L6v, p < 0.05 for the preformed C-wire group), except in the anterior region in the preformed C-wire group.
In the skeletal analysis, A and B points remodeled posteriorly because of retraction of the anterior teeth; the change was significant only at A point (PTV-A, p < 0.05) in the preformed C-wire group and B point (PTV-B, p < 0.01) in the conventional C-wire group. No significant vertical skeletal change was noted in both groups despite slight extrusion of the mandibular molars. With regard to the soft-tissue changes, the upper and lower lips moved posteriorly (UL to E-line and LL to E-line, p < 0.001 for both groups). No significant intergroup difference was observed except for the change in mandibular incisor angulation (Table 1).
DISCUSSION
Various protocols using different wires and brackets have been developed to control tooth movements, such as biometric and bidimensional systems.14,15 These systems concern posterior "play" and three-dimensional control of anterior teeth during space closure.13 Preformed C-wires are an effective option for posterior sliding mechanics and good torque control of anterior teeth while applying light alignment forces.
In this study, the null hypothesis was proved; preformed C-wires yielded similar therapeutic outcomes to conventional C-wires during retraction. However, preformed C-wires enabled initiation of leveling and space closure on the same day as bracket placement and maintenance of one archwire until the extraction spaces were fully closed, in contrast to the three or four archwires typically required to align teeth (6-9 months) before initiating retraction or space closure.15 In anterior crowding, selective or loose ligation of crowded teeth (especially the lateral incisors) and retraction of the canines with light elastics are initiated first until all of the anterior teeth are engaged on the archwire. The preformed C-wire technique with minimum retraction force reduced the risk of root resorption of the lateral incisors and as well as distal tipping of the canines. During alignment, proclination or round-tripping of crowded incisors was prevented with light elastic chains or ligature wire from the retraction hooks to the TSADs. En-masse retraction with elastics or springs from the TSADs to the retraction hooks was then performed to close the remaining extraction spaces.
Several factors influence the choice of archwire progression, such as personal preference, cost, and wire characteristics for ideal force generation. Clinicians typically use smaller round wires to generate lighter forces during the preliminary alignment stage. Rectangular superelastic NiTi archwires offer an interesting advantage. Flexural rigidity dependence on cross-sectional dimension differs from linear elasticity prediction because of martensitic transformation.16,17 The rigidity decreases with increasing deflection, and this phenomenon is accentuated in the unloading process. With NiTi alloys, flexural rigidity is not constant and the influence of size is not as important as might be expected.16,17 Therefore, in some cases, treatment can begin with rectangular wires that nearly fill the bracket slot and still deliver a force deemed to be physiologically desirable for tooth movement and compatible with patient comfort. This is the basis for using rectangular NiTi archwires as the anterior component of preformed C-wires as they offer simultaneous alignment, leveling, and torque from the beginning of treatment.
Torque control of the anterior segment is important during space closure. Torque loss of the anterior teeth and intrusion of the canines can easily occur in the sectional retraction approach. While developing the preformed C-wires, we first tried using only NiTi archwires on the anterior teeth and through the holes in the TSADs. However, the result was vertical bowing and bite deepening.18 Use of pretorqued NiTi archwires (30-45°) in the anterior section of the assembly caused labial flaring of the canines. Subsequently, we combined the non-torqued NiTi section with SS archwires for improved control of canine movements.
The vector of the retraction force (and thus, the moment applied to the anterior segment) can be altered with the height of the retraction hook and/or level of force. We found that a 7- to 10-mm-high retraction hook provides the best torque control. A longer power arm will rotate the anterior segment counterclockwise, extruding the canines.19,20 To lower the vector of the retraction force from the TSADs to the retraction hooks, crimpable stops can be placed on the retraction hooks at any level. For greater incisor intrusion, we used an overlay occlusal curve NiTi archwire anterior to the TSADs and fixed it to the central incisor area. The C-tube has an adequate hole size (0.032 inches) to accommodate both SS and overlay NiTi archwires.
With regard to the behavior of the posterior teeth during en-masse retraction, Kim et al.11 reported that maxillary and mandibular molars show some mesialization and extrusion with conventional C-wires, which is similar to our results. Use of preformed C-wires did not lead to significant mesial movement or tipping of the maxillary and mandibular molars. The BMTA had a splinting effect on the posterior teeth, effectively preventing mesialization or mesial tipping of the molars. Occasionally, some extrusion of the mandibular molars and intrusion of the mandibular anterior teeth occurred. This could be attributed to poor cooperation with the Class III elastics while leveling with the 0.018-inch reverse curve NiTi archwires.
Although patient selection was based on specific criteria, further study with a proper randomization and double-blinding process is necessary from the beginning of the experimental design phase. Root resorption of the anterior teeth should also be evaluated accurately by using cone-beam computed tomography.
CONCLUSION
Preformed C-wires combined with maxillary TSADs enabled maximum retraction of the maxillary anterior teeth and maintenance of physiologic posterior occlusions without mesialization of the molars. It shortened the overall treatment time and allowed for comparatively easy and simultaneous leveling and space closure when compared with conventional C-wires.









 XML Download
XML Download