

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
In general, orthodontic treatment focuses on improving functional occlusion and facial appearance.1 Awareness of how facial appearance affects quality of life has rapidly increased the demand for such treatment. In most cases, the motivating factors for undergoing orthodontic treatment are enhanced dental and facial aesthetics and consequently minimized psychosocial problems.2,3 Studies of oral health-related quality of life (OHRQoL) in orthodontics are important because they provide information about therapeutic needs and outcomes as well as long-term oral health improvement.4 They can also ensure better therapeutic choices based on the patient's perception.5
Self-ligating brackets are popular in orthodontics because of their proposed superior properties including low static frictional resistance, full and stable archwire engagement, improved oral hygiene, preserved anchorage, reduced chair time and therapeutic time, and prolonged therapeutic intervals.6,7,8,9 Several researchers compared therapeutic efficiency,7 friction,8 speed of archwire changes,9 therapeutic time,10 and initial alignment of the mandibular arch11 between self-ligating and conventional brackets, but the patient's views were often not considered. Further, although studies of pain and discomfort have been performed in orthodontics,12,13,14,15 OHRQoL has not been assessed in patients wearing self-ligating and conventional brackets. Such an investigation would provide specific information on how orthodontic treatment affects the patient's physical, social, and psychological well-being in daily activities. It would also improve the patient's understanding of the potential benefits and drawbacks of treatment.16
The objective of this study was to compare OHRQoL of patients wearing conventional, active self-ligating (ASL), and passive self-ligating (PSL) brackets in different therapeutic phases. The null hypothesis was that the prevalence and severity of impacts on OHRQoL would not differ among the patients in any therapeutic phase.
MATERIALS AND METHODS
Study population
This randomized controlled clinical trial included 60 Malaysian patients who visited the Faculty of Dentistry, University of Malaya, for fixed orthodontic treatment. The subjects were selected from the waiting list by purposive sampling. The inclusion criteria were age 14-24 years; Class I, II, or III skeletal pattern; moderate crowding or spacing in the maxillary and mandibular arches; and no intervention planned with extraoral and other intraoral appliances within the first 6 months of treatment. The exclusion criteria included severe skeletal disharmony requiring orthognathic surgery and presence of syndromes, dental caries, or periodontal disease.
All the subjects were given oral healthcare products (orthodontic toothbrush, fluoride mouthwash, and interdental toothbrush) and reimbursed for transportation during the study; they paid only half the total cost of the treatment. Ethical approval was obtained from the Research Ethics Committee of the Faculty of Dentistry, University of Malaya [DF OT0803/0024(P)]. This study was monitored by the local institutional review boards.
Randomization
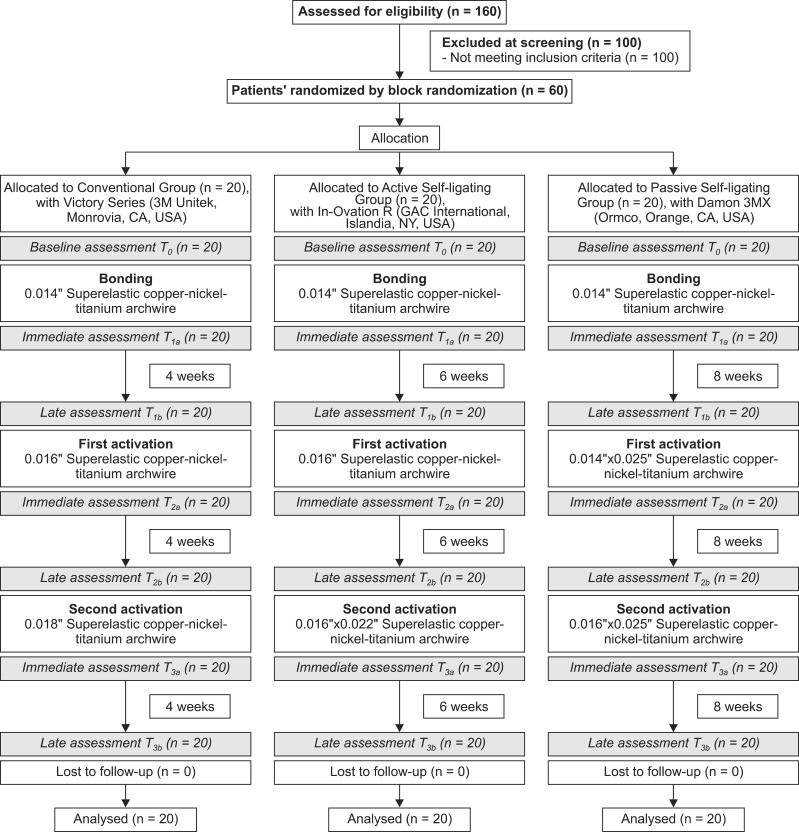
Block randomization was performed by a dental nurse to allocate the subjects to conventional (Victory Series; 3M Unitek, Monrovia, CA, USA), ASL (In-Ovation R; Dentsply GAC International, Islandia, NY, USA), and PSL (Damon 3MX; Ormco Corporation, Orange, CA, USA) groups. In brief, each patient's initials were written on a piece of paper, and the paper was randomly placed in one of three boxes representing the bracket systems. The process was repeated until all the 60 patients were assigned to a group. It ensured that the subjects had the same probability of being allocated to a group and the groups included an equal number of subjects.
Instruments
A self-administered questionnaire was developed to gather information on sociodemographics. OHRQoL was measured by using a modified 16-item Malaysian version of the Oral Health Impact Profile (OHIP-16[M]), adapted from Saub et al.17 This instrument was chosen because it is used in most studies of OHRQoL in orthodontics. It focuses on the impact of oral health on quality of life via seven domains: "functional limitation," "physical pain," "psychological discomfort," "physical disability," "psychological disability," "social disability," and "handicap." Responses to each item are scored as follows: 1 = never; 2 = hardly ever; 3 = occasionally; 4 = fairly often; and 5 = very often.
For this study, three items were added on the basis of the outcome of a pretest: "problems in speech," "problems in cleaning," and "pain." The item "have you had to spend a lot of money?" was removed because the patients were mainly schoolchildren funded by their parents. The total score ranged from 16 to 80, where 16 indicated no impact and 80 indicated the worst impact on OHRQoL.
The questionnaires were prepared in Malay and English. They were tested before data collection to check for face validity.
Intervention
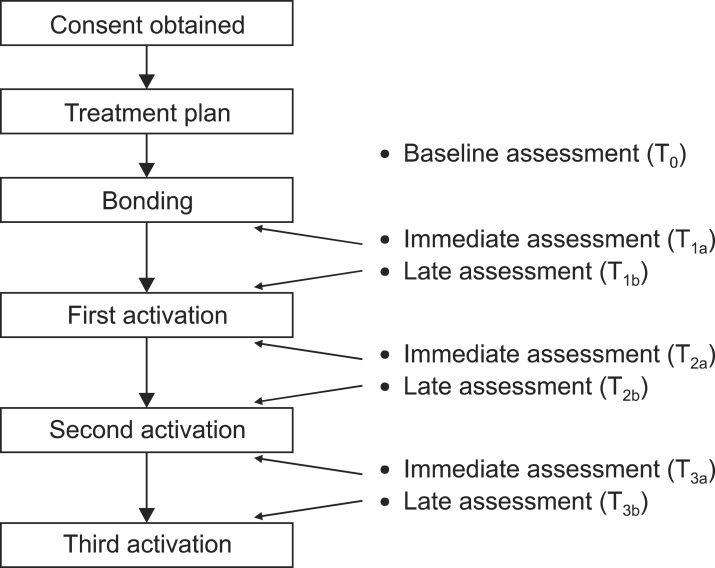
Each patient received an information sheet about the research and gave written informed consent before responding to the first questionnaire. After examination, diagnosis, and treatment planning, the patients completed the baseline questionnaire to assess OHRQoL before any intervention. At the next appointment, the brackets were bonded according to the manufacturers' protocols. Activation was performed according to the manufacturers' specifications at intervals of 4, 6, and 8 weeks in the conventional, ASL, and PSL groups, respectively.
Immediate and late assessments were conducted in the bonding, first activation, and second activation phases. For the immediate assessment, the questionnaires were given to the patients, and they mailed the completed questionnaires after the visit. The late assessment coincided with the activation appointments, minimizing patient constraints and maximizing compliance; the patients completed these questionnaires before the subsequent visit. The data collection sequence is summarized in Figure 1. The therapeutic intervals and archwire changes were standardized for every activation phase. Only one operator performed the interventions.
Statistical analysis
Two parameters of OHIP-16[M] were computed according to Locker and Quiñonez18:
i. Prevalence: the percentage of respondents reporting one or more impacts as "very often" or "quite often." This variable identifies those whose oral health impacts are chronic rather than transitory.
ii. Severity: the sum of the response scores of the 16 items, which considers impacts experienced at all frequency levels.
Because items in each domain vary, the scores were standardized to a range of 0 to 100 by using the Fayers and Machin19 formula:
where Z is the standardized score, X is the summed score, m is the number of items, and k is the response category.
The prevalence and severity values were not normally distributed. Therefore, the Kruskal-Wallis and chi-square tests were used for analyzing continuous and categorical data, respectively. p-value was set at 0.05. All measurements were analyzed using Statistical Package for Science Social version 17.0 (SPSS, Inc, Chicago, IL, USA).
RESULTS
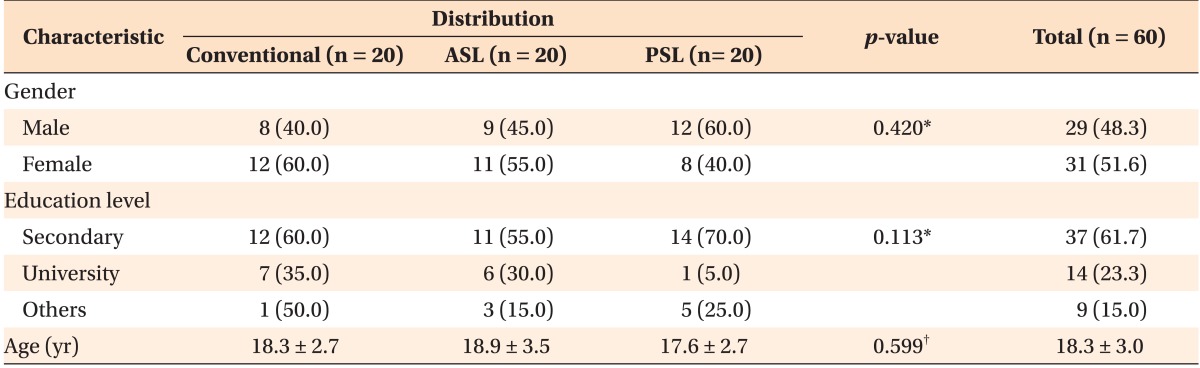
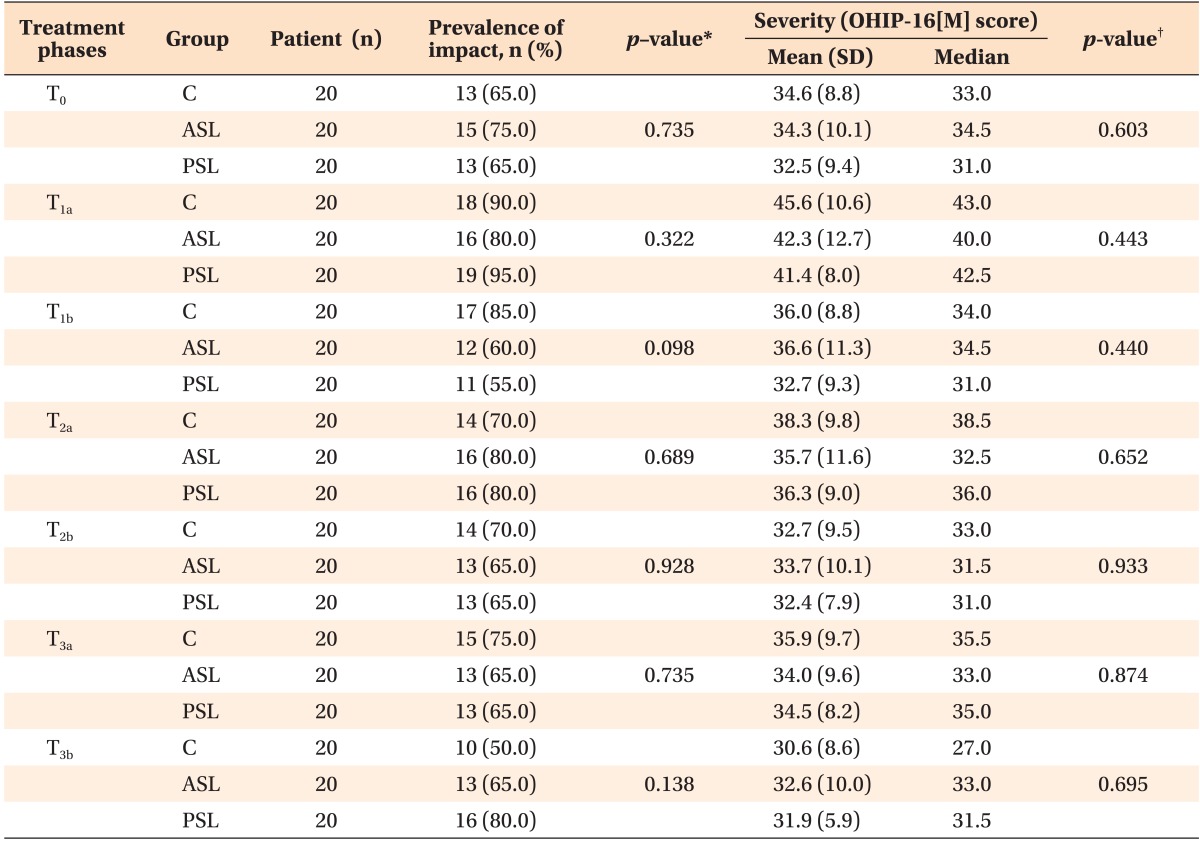
The response rate was 100% and all the subjects completed the questionnaires in all the therapeutic phases (Figure 2). The groups did not show significant differences in age, gender, and educational level (Table 1). They also did not show significant differences in the prevalence and severity of impacts on OHRQoL at the baseline and immediate and late assessments (Table 2).
The immediate impacts were more prevalent and severe than the late impacts in all the therapeutic phases regardless of the group. The bonding phase had the greatest effect; the PSL and ASL groups showed more immediate and late impacts, respectively, whereas the conventional group showed impacts in both the assessments. The first activation phase had similar impacts regardless of the assessment time. The conventional group showed more immediate impacts after the second activation, whereas the PSL and ASL groups had more late impacts in this phase.
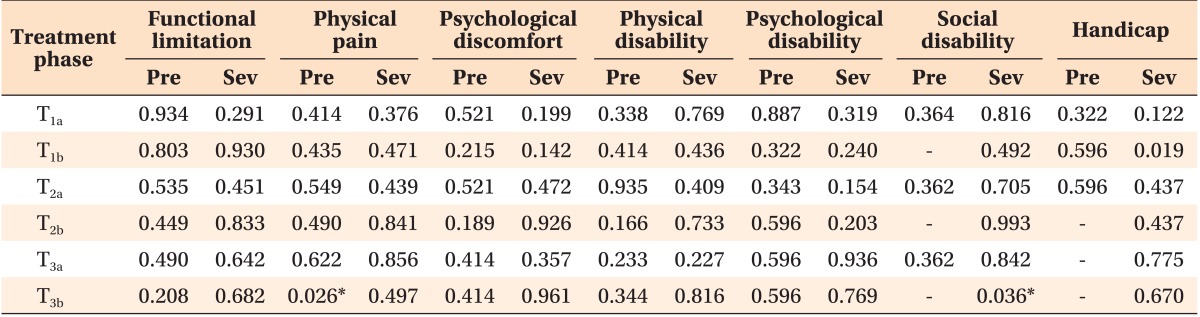
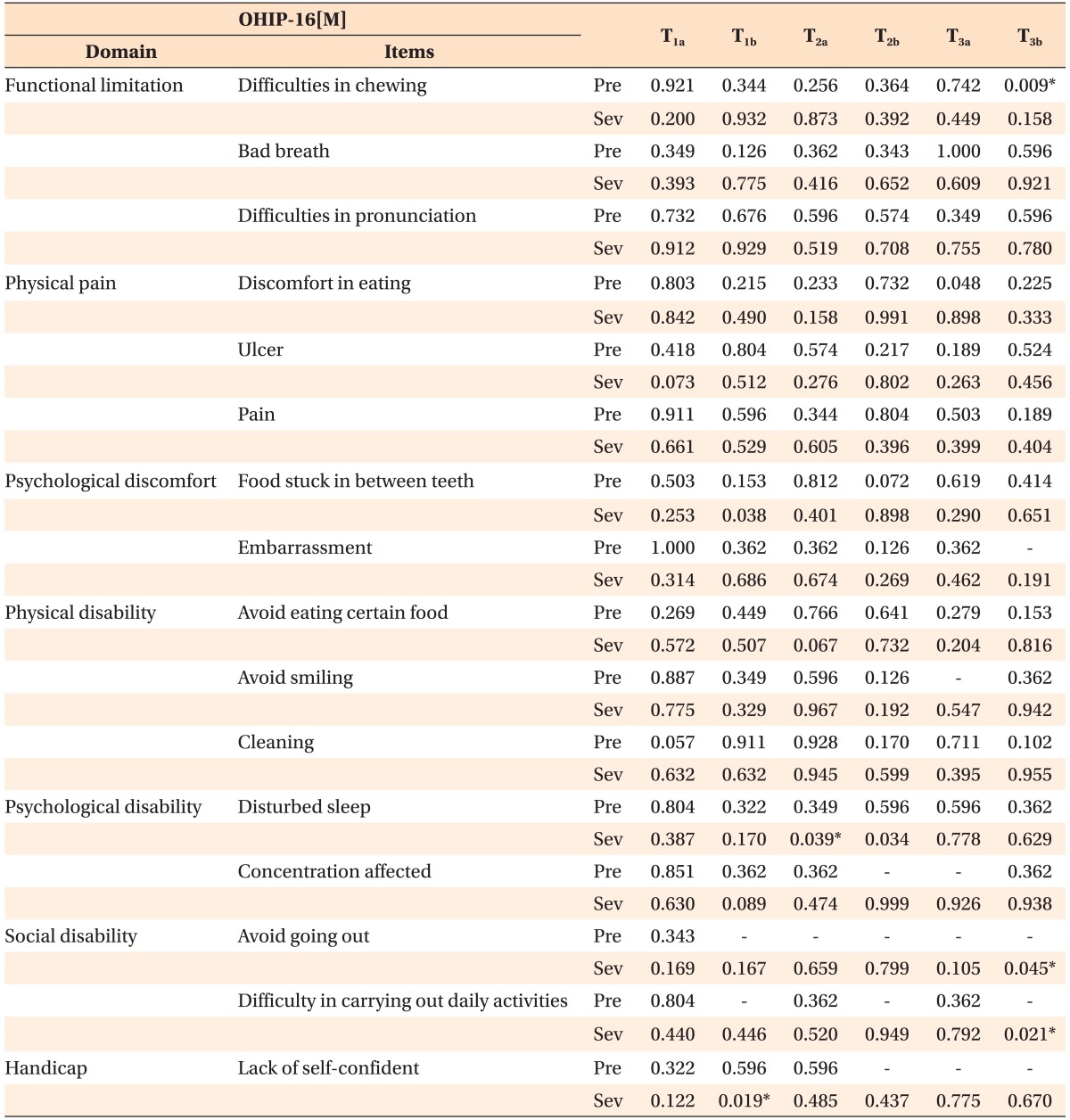
Similar OHIP-16[M] domains ("physical disability," "functional limitation," "physical pain," and "psychological discomfort") were affected in the therapeutic phases (Table 3). The "social disability" and "handicap" domains were the least affected in all the groups. Significant differences in the prevalence of "physical pain" and severity of "social disability" were noted at the late assessment of the second activation phase, with the PSL group showing the highest values. Significant differences were also observed in the severity of "food stuck between teeth" and "lack of self-confidence" at the late assessment of the bonding phase (Table 4). Further, the prevalence of "difficulties in chewing" and severity of "avoided going out" and "difficulty in performing daily activities" showed significant differences at the late assessment of the second activation phase. The PSL group had the most severe impacts according to the OHIP-16[M] items in this phase.
DISCUSSION
In this study, the absence of significant differences in the prevalence and severity of impacts on OHRQoL in any therapeutic phase among the groups proves our hypothesis.
In this study, the prevalence of impacts was quite high (65-75%) at the baseline. This value is higher than that (slightly over 50%) found by Saub and Locker20 in Malaysian adults. The difference was expected because the present subjects were patients with malocclusion who requested treatment.
In the bonding phase, PSL brackets (Damon 3MX) caused the highest prevalence of immediate impacts. This observation may be explained by the bracket shape. Major et al.21 compared the shape of In-Ovation and Damon Q brackets and found that Damon Q brackets (Ormco Corporation, Orange, CA, USA) are more rectangular, with nearly 90-degree corners between the slot bottom and the walls. Damon Q brackets are a more compatible and sophisticated version of Damon 3MX brackets. As Damon 3MX brackets are relatively bulky, the patients wearing these brackets may have felt more uncomfortable and had greater difficulty in cleaning their teeth than the other patients.
Interestingly, the subjects bonded with conventional brackets had the highest severity score, indicating poorer OHRQoL than those with self-ligating brackets. The tension and compression of the periodontal ligament during orthodontic treatment cause pain.22 This situation would be more apparent in patients with conventional brackets because of elastomeric ligatures, which produce friction that causes pain, when compared with self-ligating brackets, which are frictionless. Such pain will affect eating abilities, as reflected by the most affected domain ("physical pain") in the present study. The conventional group also reported the highest prevalence of late impacts after bonding. Although elastomeric ligatures reportedly have force decay tendencies, the failure load remained comparably high (67%) in situ even after 6 weeks.23 The late assessment of the bonding phase was performed after 4 weeks, so the effect of elastomeric ligation would still have been perceptible. The lower prevalence of impacts of self-ligating brackets may be attributable to the adaptation to the relatively bulky brackets and frictionless system. The questionnaires in the PSL and ASL groups were administered at 8- and 6-week intervals, respectively, which would have allowed the subjects to adapt to the situation.
Immediate assessment after the first activation showed that self-ligating brackets had higher prevalence of impacts than the conventional group. In this phase, the archwire was drastically changed from a small round one (0.014 inch copper-nickel-titanium) to a larger rectangular one (0.014 × 0.025 inch copper-nickel-titanium) in the PSL group. An increase in wire size would increase static frictional resistance,6 which can cause pain and discomfort. Therefore, use of rectangular archwire might have had a greater impact. However, again, the conventional group had more severe impacts, which may have been caused by the strain from elastomeric ligatures. Furthermore, the archwire in the conventional group was slightly larger (0.016 inch copper-nickel-titanium) in this phase than in the bonding phase (0.014 inch copper-nickel-titanium). All the three bracket systems caused almost similar prevalence and severity of late impacts on "psychological discomfort" and "physical disability." This finding might be explained by the adaptation to the brackets over time. Studies have shown that perceived pain peaks at around 24 hours after the placement of archwire, with reducing levels subsequently.24,25,26 This also suggests better adaptation of all patients to appliances, a phenomenon known as "learning experiences of treatment."27
At the second activation, the archwire for conventional and ASL brackets was changed from round (0.016 inch) to rectangular (0.016 × 0.022 inch) copper-nickel-titanium. Meanwhile, in the PSL group, the shape of the archwire was the same (i.e., rectangular) but a larger dimension was used (from 0.014 × 0.025 inch to 0.018 × 0.025 inch copper-nickel-titanium). In this phase, the conventional group again had the highest prevalence and severity of immediate impacts. Although this was the first instance where rectangular archwire was inserted in both the conventional and the ASL groups, elastomeric ligatures in the conventional group could have complicated the situation. Further, the prevalence of late impacts was higher in the PSL group and the domains mostly affected were "physical pain" and "psychological discomfort," with "food stuck in between teeth" being the most common effect reported. The larger archwire in the PSL group could have caused food to become trapped between the archwire and the teeth, causing discomfort. The severity of impacts was the highest in the ASL group, which could be due to the sustained friction in this system, compared with conventional brackets, which might show forced decay of elastomeric ligatures.
This study has several limitations in terms of sample size and administration of questionnaires. Strict inclusion and exclusion criteria were used to optimize group homogeneity, because factors such as age and severity of malocclusion play a role in the reporting of impacts on OHRQoL.28,29 Block randomization was performed to ensure an equal number of subjects per group, because pooling of eligible patients would have been time consuming given the stringent inclusion criteria. Although the small number of participants in each group could cause bias, the operator had no control over the responses, so the bias may not be significant. Further, the bracket systems in this study had different manufacturer-specified therapeutic intervals, which could have introduced bias, because a longer interval would have allowed adaptation to the appliance and thus affected the reporting of OHRQoL. The sample was initially planned to ensure 30 patients per group, as proposed by Roscoe.30 However, because of the stringent inclusion criteria and required therapeutic time, only 20 patients could be recruited in each group. The estimated statistical power by the post-hoc test was 74% for a sample size of 60, divided into three groups, with medium effect.
CONCLUSION
Within the study limitations, we conclude that no bracket system offers superior OHRQoL. Patients may experience some impacts in the initial therapeutic phase. These findings would be useful when clinicians want to modify the standard protocol of the manufacturers, such as the archwire sequences or therapeutic intervals, to achieve patient comfort, as long as treatment is not jeopardized. They could also be applied when explaining the therapeutic phases, especially the initial one, and selecting the optimal bracket system based on the patient's preference.
 XML Download
XML Download