

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Nowadays, clinicians tend to apply lighter forces during orthodontic treatment by means of self-ligating brackets and small superelastic archwires. However, because superelastic archwires are preformed, they may be difficult to adapt to a patient's unique arch form. Failure to maintain the arch form increases the probability of relapse.1-6 In this regard, correct identification of the arch form is very important for achieving a stable, functional, and esthetic outcome.
Several classification methods using incisal edges and cuspal tips as landmarks have been developed to evaluate arch forms.1-7 Clinical bracket points have also been used as landmarks for mandibular arch form assessment.8,9 Unfortunately, these methods are not sufficiently accurate to allow proper placement of superelastic archwires. On the other hand, Camporesi et al.10 evaluated the average arch form through three-dimensional (3D) derived facial axis (FA) points, which correspond to bracket points and are more relevant to clinical practice. Further, Bayome et al.11 suggested a new classification of arch form based on FA points.
Arch size and arch form tend to differ among ethnic groups.7-9,12-18 The distribution and dimensions of the arch forms of Korean subjects were found to be different from those of other ethnic groups.8,9,11,12,14 Nevertheless, the average arch form of Vietnamese people, who originated from a homogeneous ethnic background to Korean people in Southeast Asia, has not yet been assessed. Moreover, no comparative studies of arch forms have been conducted between these ethnic groups by using FA points as landmarks on 3D models.
The purpose of this study was to compare the mandibular arch forms of Korean and Vietnamese patients by using FA points on 3D models.
MATERIALS AND METHODS
Subjects
The Korean population consisted of 68 patients (mean age, 22.6 years), with Class I (n = 30) and Class II (n = 38) malocclusion, from the Department of Orthodontics, Seoul St. Mary's Hospital, The Catholic University of Korea (Seoul, Korea). The Vietnamese population comprised 78 patients (mean age, 17.3 years), with Class I (n = 41) and Class II (n = 37) malocclusion, from the Department of Orthodontic, Faculty of Odontostomatology Medicine, Hanoi University, and private clinics in Hanoi and Ho Chi Minh City. The institutional review board of The Catholic University of Korea approved this study (MC12SSS10073).
The inclusion criteria were as follows: complete permanent dentition excluding the third molars; normal tooth size and shape; absence of supernumerary teeth; 3 mm or less of arch length discrepancy; no restorations extending to the contact areas, cuspal tips (incisal edges), or cervical areas; and no previous orthodontic treatment.
Digitization
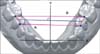
Mandibular casts of the subjects were scanned in their occluded relationships by using a 3D laser scanner (KOP-300; Orapix Co. Ltd., Seoul, Korea) at 20-µm resolution. The FA point19 of each tooth was digitized on the 3D models by using Rapidform 2006 software (INUS Technology Inc., Seoul, Korea) (Figure 1).
The transverse and anteroposterior directions were set as the X-axis and Y-axis, respectively, and the line perpendicular to these planes was marked as the Z-axis. The contact point of the central incisors was considered the origin of the coordinates. The original X-axis was adjusted so that it was parallel to the mean inclinations of the lines connecting the bilateral contact points of the first and second premolars (line A) and the second premolars and first molars (line B). The Z-axis values were nullified (Figure 2).
Measurements
Four linear measurements were calculated for each arch form (Figure 3): intercanine width, the distance between the canine FA points; intermolar width, the distance between the first molar FA points; intercanine depth, the shortest distance from the line connecting the canine FA points to the origin; and intermolar depth, the shortest distance from the line connecting the first molar FA points to the origin. The intercanine and intermolar width-to-depth ratios were also calculated.
In addition, arch form images were printed on a 1:1 scale and compared with arch form templates (OrthoForm; 3M Unitek, Monrovia, CA, USA) to select the arch form that best fit the eight FA points from the right to the left first premolars. The subjects were then grouped according to the arch form (tapered, ovoid, and square) and the frequency distributions of each arch form in both the ethnic groups were calculated.
To assess the measurement error, 10 randomly selected models from each group were analyzed after two weeks to evaluate intra-operator variability. The intraclass correlation (ICC) test revealed high reliability between the assessments (ICC > 0.8). The arch forms were also classified twice by the same examiner. The difference between the evaluations was analyzed by the Wilcoxon signed-rank test and found to be negligible (p > 0.05). Therefore, the first classification was used. For confirmation, a second examiner classified 30 arch forms from each ethnicity. The agreement between the examiners was high (kappa = 0.898). Both the examiners were blinded to the groups.
Statistical analysis
Statistical evaluation was performed with SPSS 16.0 software (SPSS Inc., Chicago, IL, USA). The chi-square test was used to analyze the association between arch form and ethnicity. Multivariate analysis of covariance (MANCOVA) was performed to compare the gender-adjusted means of the arch measurements according to ethnicity, arch form, and Angle's classification of malocclusion. All analyses were tested at the significance level of 0.05.
RESULTS
Square arches were the most common in the Korean and Vietnamese groups (44% and 62%, respectively), followed by ovoid (29% and 27%, respectively) and tapered (27% and 12%, respectively) arches (Figure 4). The frequency distributions of the arch forms within the ethnic groups were significantly different (p = 0.038; Table 1). Square arches were significantly more common in the Vietnamese group (p < 0.001). The Korean group showed even distribution of the three arch forms (p = 0.161).
In the multivariate analysis of the arch measurements according to ethnicity and Angle's classification of malocclusion, arch form (p < 0.001), ethnicity (p = 0.001), and type of malocclusion (p = 0.024) had significant main effects. Gender showed no significant effect (p = 0.19). Further, no significant interaction was noted between ethnicity and type of malocclusion (p = 0.056). Intercanine and intermolar widths showed no significant differences according to ethnicity and type of malocclusion. However, intercanine depth and intercanine and intermolar width-to-depth ratios demonstrated significant differences between the ethnic groups. Intermolar depth was significantly different according to Angle's classification of malocclusion (Table 2).
In the multivariate analysis of the arch measurements according to arch form and ethnicity, both arch form (p < 0.001) and ethnicity (p = 0.002) had significant main effects. Gender (p = 0.16) and Angle's classification of malocclusion (p = 0.23) had no significant effects. No significant interaction was observed between ethnicity and arch form (p = 0.054). Further, intercanine width showed no significant difference, but intercanine depth and intercanine and intermolar width-to-depth ratios again demonstrated significant differences. Intermolar depth and width were also significantly different: the Vietnamese group had significantly narrower intermolar width in the tapered and ovoid arches, and the square arches of the Korean group showed significantly less intermolar depth (Table 3).
DISCUSSION
Great technologic strides in communication and transportation over the past few decades have contributed to rapid globalization and widespread flow of people. Therefore, it is appropriate to examine and compare the morphologic features of ethnic groups from various parts of the world.
The population of Vietnam is reportedly 92.5 million.20 The Vietnamese population in Korea has reached over 160,000 and is rapidly increasing.21 However, until now, research on Vietnamese arch forms has not been conducted. Therefore, we aimed to identify the average arch form of Vietnamese people and clarify the morphologic differences in the mandibular arches between Vietnamese and Korean populations.
McLaughlin and Bennett5 classified arch forms into 3 main types: tapered, ovoid, and square. Several mathematical methods have been applied to depict arch forms.1,10,11 However, the accuracy of arch form identification by using incisal edges and cuspal tips1,2,7-9,22-28 or clinical bracket points as landmarks on two-dimensional photocopies of casts is doubtful because of the failure to digitize FA points. In our study, FA points were used on 3D models for evaluating and classifying arch forms because of their high accuracy.29,30
In this study, the Vietnamese population had greater arch depth but not significantly different arch width from the Korean population. Kook et al.8 showed that Caucasians have a narrow arch but not significantly different arch depth compared with Korean people, which suggests that Vietnamese people have the deepest arches and Caucasians have the narrowest ones among the three ethnic groups.
Previous studies demonstrated that the most common arch form is tapered in Caucasians (43.8%), square in Korean and Japanese people (46.7% and 45.6%, respectively), and ovoid in Israeli people (50.7%).8,9,15 Meanwhile, Bayome et al.12 reported an even distribution of the arch forms in Egyptians. In our study, square arches were the most common in the Vietnamese group (62%), followed by the ovoid and tapered arches; on the other hand, the Korean subjects showed an even distribution of the arch forms. These differences are attributable to genetic and environmental factors. Class III malocclusion cases were not included in this study; this type of malocclusion might have decreased the percentage of the square arch form.
This study was the first comparison of Vietnamese and Korean arch forms. The sample size was not large enough to evaluate the frequency distributions of the arch forms in Class I and II malocclusion cases. Further, Class III malocclusion cases are difficult to find in Vietnamese people. Further research using cone-beam computed tomography in a larger sample size including Class III malocclusion cases is recommended for evaluating the clinical and basal arch forms.
CONCLUSION
Vietnamese people tend to have deeper and wider arches than Korean people. The three arch forms are evenly distributed in Korean people, but Vietnamese people frequently have square arches. Clinicians should identify the arch form of each ethnic group before initiating orthodontic treatment.






 XML Download
XML Download